John E Rush, DVM, MS, DACVIM (Cardiology), DACVECC
INTRODUCTION
Thoracic radiographs are a key element of diagnostics in veterinary cardiology. Radiography offers information that is complimentary to physical examination, echocardiography, electrocardiography, and cardiac biomarkers. Thoracic radiographs are also key in making several important therapeutic decisions. If you ever get the chance to work with a cardiologist or radiologist trained in the pre-echocardiogram era you will amazed at the information they are able to extract from a radiograph!
The ability to effectively interpret radiographs of the cardiovascular system requires a collective understanding of normal radiographic anatomy, the pathophysiology of the various cardiac diseases and the ability to detect and interpret radiographic abnormalities. Much of this lecture will concentrate on dogs and cats, since thoracic radiographs for cardiac disease are a bit less commonly done in other species.
OBJECTIVES
1. Be able to measure and assess cardiac silhouette size
a. Recognize the breed variation in cardiac silhouette shape and relative size
b. Be familiar with “rules of thumb” for assessing cardiac silhouette enlargement including:
- %
thoracic cavity on DV view; Number of Intercostal spaces on the lateral view
- Vertebral heart score – be able to measure VHS from the lateral view
c. Be able to recognize an enlarged and a small cardiac silhouette
2. Assessment of cardiac silhouette location & shape
a. Identify where the cardiac chambers are on a lateral and dorsoventral radiograph
b. Explain cardiac chamber location and use the “Clock face analogy”
c. Be able to point to the cardiac apex and the location of the cardiac “waist”.
d. Recall normal variations in cardiac silhouette shape resulting from patient positioning
- Dorsoventral
vs. ventrodorsal
- Right lateral vs. left lateral
e. Recognize a globoid cardiac silhouette shape and the explain the pathologic significance
f. Recognize variations in cardiac position and shape resulting from non-cardiac diseases
- Pectus
excavatum, Lung collapse (atelectasis), Pneumothorax
- Peritoneopericardial diaphragmatic hernia (PPDH)
3. Assessment of the normal location and size of the pulmonary and thoracic vasculature
a. Know the anatomy of pulmonary artery, bronchus and pulmonary vein.
b. Assess pulmonary vessel size using anatomic landmarks.
c. Label the location of aorta, cranial and caudal vena cava on a thoracic radiograph
4. Assessment of common pleural and pulmonary manifestations of cardiac disease
a. Recognize the appearance of pulmonary edema and pleural effusion
b. Be able to identify alveolar pattern, bronchial pattern, interstitial pattern, and pulmonary over-circulation or under-circulation
Assessment of cardiac silhouette size
Introduction:
The term cardiac silhouette is often used because on thoracic radiographs we cannot distinguish the soft tissue densities of myocardium vs blood in the cardiac chambers vs pericardial fluid or the pericardium itself.
1. Non-pathologic variations in cardiac silhouette size (and shape):
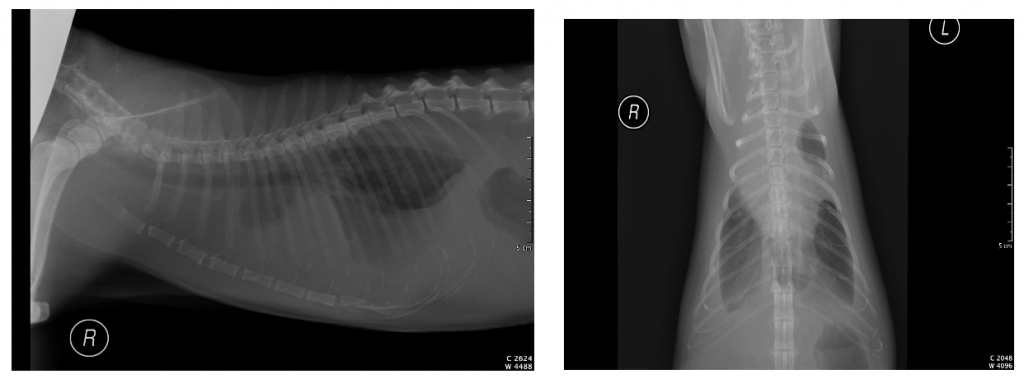
Cogs come in a wide variety of shapes and sizes and thus the chest conformation and the cardiac silhouette has an array of normal appearances. For example (see below) there is a comparison of right lateral radiographs from a normal German shepherd (left) and a normal English bulldog (right). As you can see the cardiac silhouettes and other thoracic structure have quite different appearances. The heart of the German shepherd is relatively tall and narrow, while the English bulldog heart is more rounded and the cranial border is difficult to define due to normal cranial mediastinal fat. Some general rules of thumb: Deep chested breeds (e.g. German shepherds, Irish setters) will have a tall and narrower looking cardiac silhouette that occupies less of the thoracic cavity. Compressed or muscular breeds (e.g. Bulldogs, Dachshunds, Jack Russell terriers) will have more rounded cardiac silhouettes that appear to have right-sided enlargement radiographically (even though the right heart is a normal size) and occupy a greater volume of the thoracic cavity. The Vertebral Heart Size (or Vertebral Heart Score, also called VHS) is one test that can help in evaluating cardiac size between breeds, although there is some breed-to-breed variation in VHS.

The good news is that cats are a relatively homogenous population in terms of body size and shape. Therefore, the same is true for their cardiac silhouettes. i.e. we can expect a normal heart in a Cornish Rex to appear like that of a domestic short hair.
2. Assessment of cardiac silhouette enlargement (overall cardiomegaly):
We often assess cardiac silhouette shape and size together when trying to determine the presence of cardiac disease. The subjective assessment of cardiac enlargement relies upon how much space the heart occupies within the thoracic cavity. However, this assessment is difficult due to the large variation in canine breed conformation, variation due to patient positioning and the influence of the phase of the cardiac and respiratory cycles. Several non-pathologic factors can have a small influence the appearance of the cardiac silhouette including certain sedative drugs (e.g. Dexmedetomidine, resulting in increased size in cats), the phase of the cardiac cycle at the time of image acquisition (size: diastole > systole), choice of lateral view (size: right>left) presence of increased pericardial fat (size increased) and age-related changes in heart position in cats (horizontal orientation with increasing age in some cats). In order to help there are several crude estimates described to assess for cardiomegaly.
Rules of thumb using thoracic cavity dimensions to compare the cardiac silhouette size.
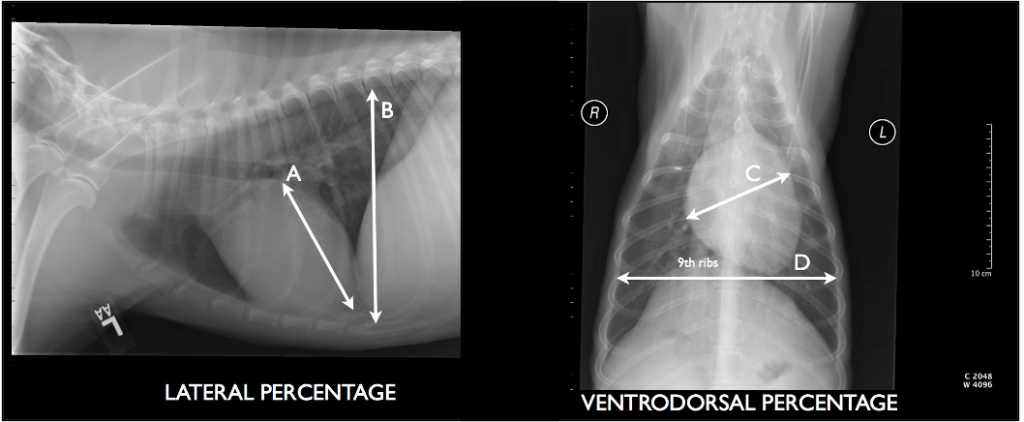
a. Lateral view: base to apex cardiac silhouette height (A) < 60% of the total dorsoventral thoracic cavity height (B)
b. Ventrodorsal view: Cardiac silhouette width (C) < 50% of pleura to pleura width at level of 9th rib (D)
An alternative index is to use the number of intercostal spaces on the lateral view as the baseline to compare the cardiac silhouette size.
a. Dogs: 2.5 to 3.5 intercostal spaces
b. Cats: Cardiac width < 2.0 to 2.5 intercostal spaces
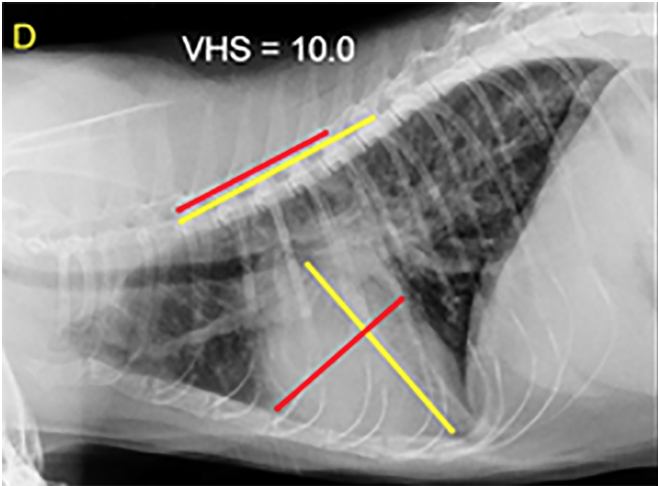
The Vertebral Heart Score (VHS) is used to come up with a more objective measure of cardiac silhouette size that was independent of dog breed conformation. Despite the original aim of a value independent of conformation and athletic condition, some breed specific reference ranges have since been identified in dogs. Regardless, the VHS is often used by cardiologists for making therapeutic decisions, especially in dogs with pre-clinical mitral valve disease. Progressive increases in VHS over time can be used as a means to assess disease progression and help predict the onset of heart failure.
The value is calculated by measuring the long axis (L) from the carina to the apex of the heart. This is then converted into vertebral body lengths starting at the cranial aspect of T4. The maximal short axis is measured perpendicular to the long axis in the middle third of cardiac silhouette, with the caudal aspect of the line ending at or near the bottom of the caudal vena cava. These short and long axis values are measured as the number of vertebral body lengths, starting at the cranial aspect of the 4th vertebra. The vertebral short axis and vertebral long axis values are added to give the total vertebral heart score. The procedure has also been described in the ventrodorsal or dorsoventral projections.
a. Cats < 8.0 vertebral lengths (mean 7.5)
b. Dogs ≤10.5 vertebral lengths (mean 9.7)
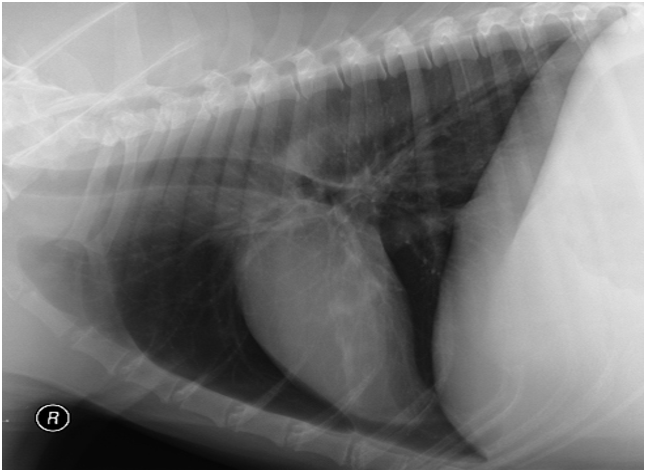
A small cardiac silhouette size (microcardia) can be seen Addison’s disease or situation of hypovolemia or many forms of shock. The cardiac silhouette is abnormally small and pointed, the ventricles appear narrower and the apex loses contact with the sternum. The thoracic blood vessels may appear small and the lungs hyperlucent (see below).
Assessment of specific cardiac chamber enlargement:
A working knowledge of the anatomy of the various chambers of the heart is important. Identifying specific cardiac chamber enlargement will help you arrive at some relatively specific differential diagnoses. The following cartoon illustrations will give you an approximate idea where the various cardiac chambers are located.
The right atrium and cranial and caudal vena cava and azygous vein:

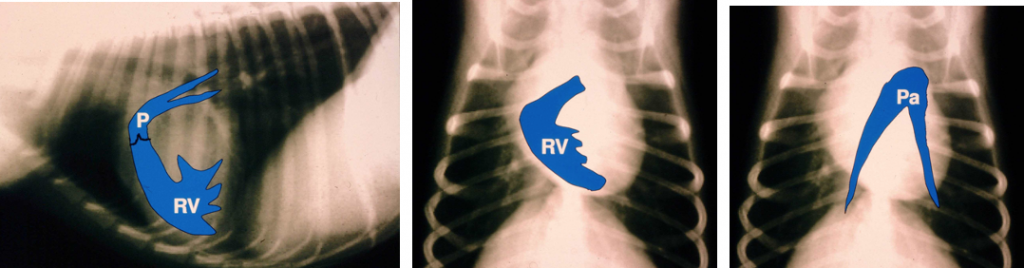
The right ventricle, pulmonic valve and proximal pulmonary artery:
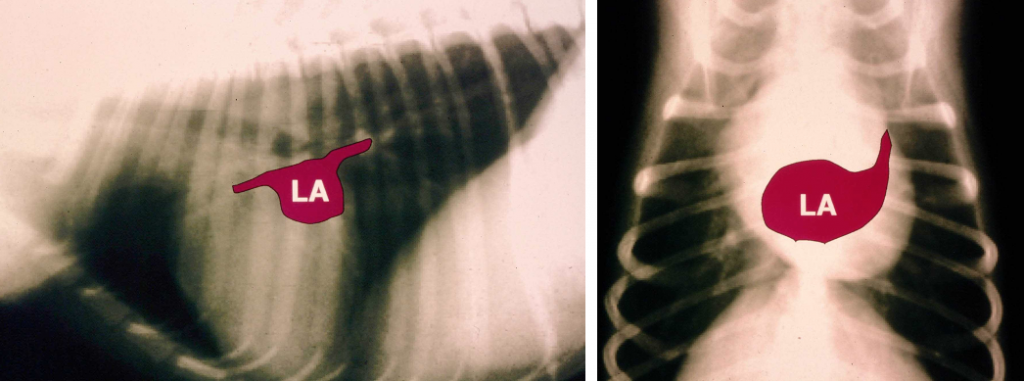
The left atrium and pulmonary vein:
The left ventricle and aorta:

Sometimes a picture is worth 1000 words – in case the pictures above didn’t help, a few words: Which side of the heart is big – the left heart or the right heart? – This can be difficult to determine, but on the lateral view the left heart occupies the caudal aspect, with the left atrium in the caudodorsal region. Especially in dogs, left atrial enlargement is usually present in dogs with pulmonary edema of cardiac cause. Conversely, the right heart is found more in the cranial and cranioventral regions on the lateral view. The more that there is right heart enlargement, without left atrial enlargement, the less likely the dog has left-sided CHF (pulmonary edema). For the DV/VD view, the heart is often likened to a clock face, and structures are noted relative to the position of numerals on the clock face. The aorta is located at the 12-1:00 location, the pulmonary artery at the 2:00 location, the left auricular appendage at the 2-3:00 site, and the left ventricle usually spans from the 3 to 5:30 or 6:00 location. The right ventricle spans from 5-6:00 site to the 9:00 position and the right atrium usually accounts for changes in the cardiac silhouette at the 9-11:00 spot. On the lateral view, the heart can roughly be divided into quadrants by a drawing a line from the carina to the left ventricular apex, with a second line perpendicular to the first which bisects the heart from top to bottom. With this scheme, the left atrium sits in the caudodorsal quadrant, the left ventricle in the caudoventral quadrant, the right atrium in the craniodorsal quadrant, and the right ventricle in the cranioventral quadrant. When looking at the vertical line from carina to apex, when there is considerably more heart cranial to this line the right heart enlargement in present. Left atrial enlargement is almost always notable in dogs with left sided congestive heart failure (pulmonary edema).


We often refer to certain locations in the heart, such as the apex or the waist of the heart, on thoracic radiographs. The “apex” of the heart is the region where the interventricular septum and left and right free wall intersect. Radiographically it is located adjacent to the caudal aspect of the sternum, ventral aspect of the heart normally, on the lateral projection. On the ventrodorsal view the apex is located in the “5 o’clock” position. A change in position of the apex can be a useful indicator of a change of cardiac shape or position. The “caudal waist” refers to the left atrium at and above the left ventricle, just below the caudal aspect of the trachea and above the caudal vena cava. The caudal waistline is lost when there is left atrial enlargement. Enlargement of the cranial aspect of the heart (cranial waist) can occur due to right atrial enlargement, pulmonary artery enlargement, enlargement of the aorta, or a mass at the heart base or attached to the right atrium.
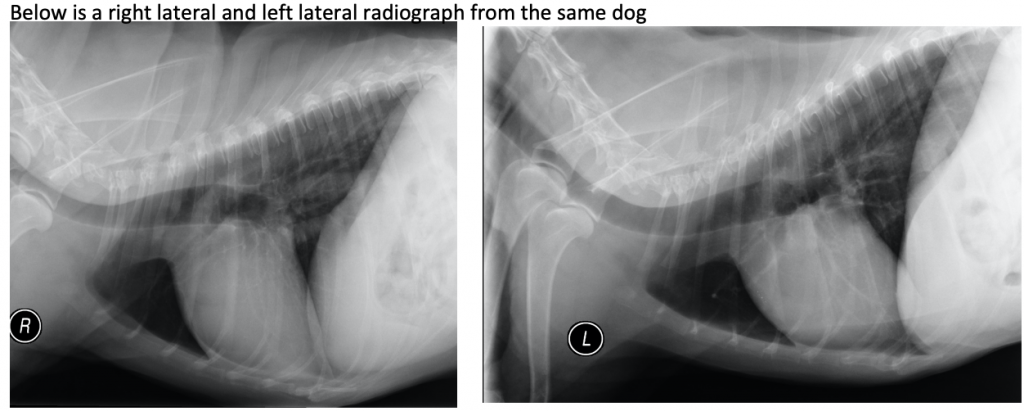
Patient positioning can affect the cardiac silhouette. Another variable that can alter the appearance of the cardiac silhouette is the position of the animal relative to the cassette/x-ray tube. For a lateral projection of the thorax we can choose either a right lateral (right side down) or left lateral (left side down) view. In the orthogonal projection we can choose either dorsoventral (sternal recumbency i.e. sternum on the table) or ventrodorsal (dorsal recumbency i.e. spine against the table) projections. These changes in position can have subtle effects on the appearance of the cardiac silhouette.
Left Lateral vs. Right Lateral: On the left lateral view the heart may have a slightly more rounded appearance, especially cranially, and this can be mistaken for right heart enlargement. The caudal vena cava can usually be seen to overlie the heart on the left lateral, while it usually “ends” at the back of the heart radiographically on the right lateral. In general, the right lateral view is preferred for evaluating the heart, at least in our clinic.
Ventrodorsal vs. Dorsoventral: In the dorsoventral projection the heart’s long axis appears shortened and the heart seems rounder (vs. elongated and narrow on the ventrodorsal projection). The caudal pulmonary vessels are easier to identify in the dorsoventral view. The differences will vary with dog breed and conformation. The appearance of the diaphragm is often stressed by radiologists (i.e., Mickey Mouse or not to tell DV vs VD), but I find these to be less predictable and considerably less useful – besides, the radiograph should be appropriately marked, so this is really just an opportunity to say “Mickey Mouse” during your education and get away with it.

A globoid cardiac silhouette: Identification or an enlarged and globoid (very spherical or rounded) cardiac silhouette on thoracic radiographs (see below) should raise the possibility of pericardial effusion (e.g. a bleeding right atrial tumor, or heart base mass like chemodectoma, etc). Unfortunately, this appearance is not 100% specific for pericardial disease, as generalized cardiomegaly (especially right heart enlargement) can also create a very rounded cardiac silhouette. Echocardiography is the best test to confirm the presence of pericardial effusion

Variations in cardiac silhouette shape and position from non-cardiac disease: A change in cardiac appearance does not always indicate cardiac disease. Non-cardiac conditions can alter the shape/appearance of the heart on radiographs. Below are some examples of conditions that alter the radiographic appearance of the heart without accompanying heart disease.
- Pectus excavatum
- A congenitally dorsally malformed sternum results in cranial and dorsal displacement of the cardiac silhouette in the lateral view and left or right lateral displacement of the heart in the dorsoventral view.

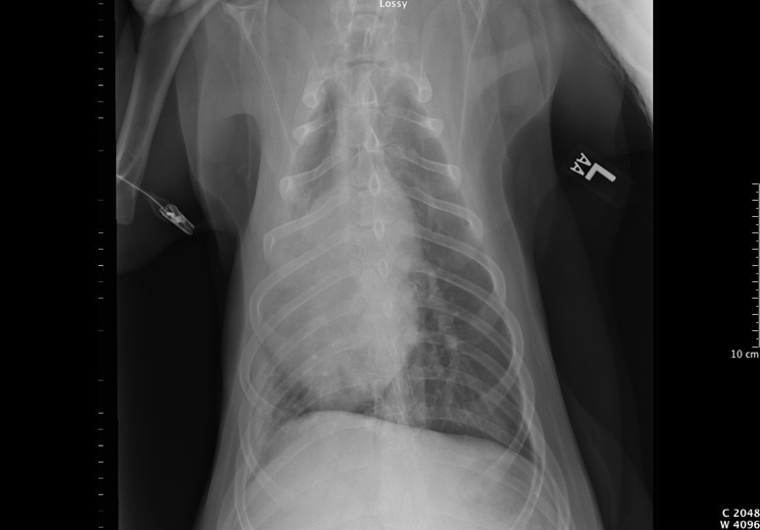
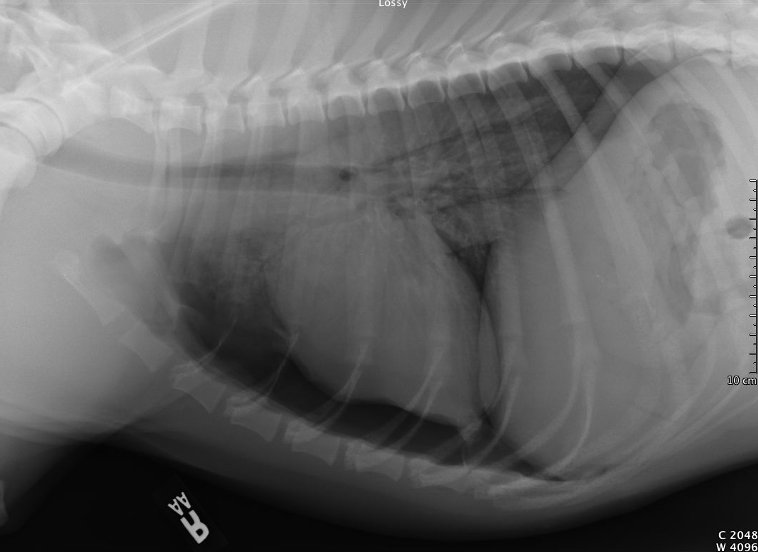
- Lung collapse (atelectasis)
- The lack of normally inflated lungs allows the heart’s position to move from midline towards the side of the lung collapse. This can happen in dogs that have been recumbent (see example below from a dog under general anesthesia – the right middle lung lobe has collapsed, and the cardiac silhouette has displaced to the right.
- Pneumothorax
- Pneumothorax will cause a separation (by a gas lucency) of the cardiac silhouette apex from the sternum in the lateral view. The dependent lung is less inflated because of the free pleural gas and is less able to support the heart in lateral recumbency.
- Peritoneopericardial diaphragmatic hernia (PPDH)
- Cats and dogs can have this congenital malformation of their diaphragm, where organs (liver, spleen, intestines) and tissue (mesenteric fat) from the peritoneal space pass into the pericardial space. The cardiac silhouette of the cat below is severely enlarged due to fat and part of the liver (as well as the normal heart) occupying the pericardial sac.

Normal location and size of the pulmonary and thoracic vasculature:
- Anatomy of pulmonary arteries and veins: Abnormalities of the pulmonary and thoracic vasculature can be encountered in a wide variety of diseases. A working knowledge of their anatomy is required so we know where to look for them.
- The Pulmonary Arteries: The main pulmonary artery segment is located at the 1 – 2 o’clock position on the clock face on the DV/VD view. This main pulmonary artery then branches into a left and right pulmonary arteries and there is subsequent branching into the lobar arteries.
- The pulmonary arteries and pulmonary veins travel alongside the bronchi. The anatomic relationship of the artery, bronchus and vein is consistent. In the lateral projections the artery is located dorsal to the bronchus and the corresponding pulmonary vein is ventral to the bronchus. In the ventrodorsal or dorsoventral views the artery is located lateral to the bronchus and the corresponding pulmonary vein is medial to the bronchus. The pulmonary veins empty into the left atrium.
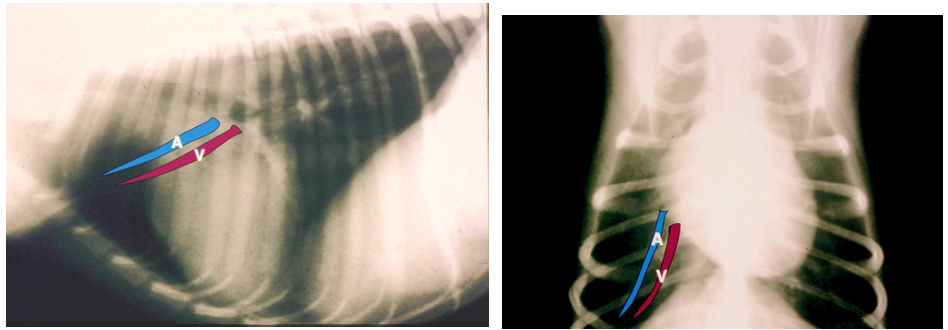
Measurements of pulmonary vessel size: On the lateral radiographs the cranial lobar artery and vein are most commonly assessed. Their diameter is considered excessive if it is greater than the smallest diameter of the 4th rib.
On the dorsoventral / ventrodorsal radiograph the point of intersection of the caudal lobar arteries and veins with the 9th rib is used. The diameter of the artery and vein caudal to the rib should not exceed the 9th rib diameter.
Normal ratio of pulmonary artery to vein diameter: The pulmonary artery diameter and corresponding pulmonary vein diameter (measured at the same level) should be approximately 1:1 in the dog. The identification of pulmonary artery enlargement alone, pulmonary vein enlargement alone or both artery and vein enlargement / size reduction, will influence your differential diagnosis list.

Anatomy of aorta, main pulmonary artery, cranial vena cava and caudal vena cava: The aortic arch is located at the 11 – 1 o’clock positions on the ventrodorsal “clock face” view. The descending aorta can be followed within the caudodorsal thorax, just to the left side of the vertebral column. In older cats you may see a cranial rotation of the cardiac silhouette with a resultant increase in sternal contact with the cranial border of the cardiac silhouette, a “bulge” in the region of the aortic arch as well as slight tortuosity of the aorta. The cranial and caudal vena cava: Normally the caudal vena cava has a variable diameter depending on the phase of the cardiac cycle and patient hydration. Enlargement of the caudal cava can indicate right heart failure or fluid overload. A small caudal vena cava can be seen with hypovolemia or shock. The cranial vena cava is usually “hidden” in the mediastinum on thoracic radiographs and cannot be easily seen.
Common pulmonary and pleural manifestations of cardiac disease:
Radiographs are routinely used in cardiac patients to assess the presence and severity of heart failure.
- Pulmonary edema:
- Pulmonary edema is the transudation of fluid from the capillaries into the interstitial space of the lungs. As fluid is a soft-tissue opacity this results in an increased opacity (“whiteness”) in the lungs. We can further describe this increase in opacity by assessing the conspicuity of the pulmonary vessels. If the pulmonary vessels are harder to see than normal, but can still be seen, we consider this to be an interstitial lung pattern. If fluid continues to leak, the fluid will overflow the interstitial space and the alveoli start to fill. The result will be the inability to see the pulmonary vessels. We call this an alveolar lung pattern. You may also see air-bronchograms (air filled airways) as part of an alveolar lung pattern. (Please see your diagnostic imaging course for a more comprehensive review of lung patterns).
The most common cause of pulmonary edema in cats and dogs is left-sided heart failure. Along with cardiomegaly, an enlarged left atrium and pulmonary venous enlargement, the distribution of the interstitial or alveolar lung pattern can help support the diagnosis of heart failure. In dogs cardiogenic pulmonary edema is typically bilaterally distributed in the perihilar region, extending peripherally especially to the cuadodorsal lung fields. The cardiac silhouette is moderately enlarged with evidence of left atrial enlargement. Although hard to appreciate on these small images, there is moderate increase in soft tissue opacity within the lung fields in the perihilar region. In combination with the cardiac changes, the lung pattern is most likely the result of cardiogenic pulmonary edema.
Cats once again prove that they are not small dogs. The distribution of cardiogenic pulmonary edema in cats can be patchy, asymmetric and involved any of the lunge lobes (see below).
- Pulmonary edema is the transudation of fluid from the capillaries into the interstitial space of the lungs. As fluid is a soft-tissue opacity this results in an increased opacity (“whiteness”) in the lungs. We can further describe this increase in opacity by assessing the conspicuity of the pulmonary vessels. If the pulmonary vessels are harder to see than normal, but can still be seen, we consider this to be an interstitial lung pattern. If fluid continues to leak, the fluid will overflow the interstitial space and the alveoli start to fill. The result will be the inability to see the pulmonary vessels. We call this an alveolar lung pattern. You may also see air-bronchograms (air filled airways) as part of an alveolar lung pattern. (Please see your diagnostic imaging course for a more comprehensive review of lung patterns).

- Pleural effusion
- Pleural effusion can occur as the result of heart failure or many other diseases. The radiographic features of pleural effusion include: widened soft tissue opacity interlobar fissures, retraction of the lung lobes from the thoracic wall, increased opacity adjacent to the sternum with a scalloped margin on the lateral views, blunted costophrenic sulci, and reduced visualization of the heart and diaphragm. With a large volume of pleural fluid the heart is difficult to see and cardiac size is difficult to evaluate. The example below shows pleural effusion in a cat diagnosed with heart failure.
Advanced cardiovascular imaging techniques:
Computed tomography (CT) and magnetic resonance imaging (MRI) can be used for cardiac imaging in our veterinary patients. These techniques are expensive and require general anesthesia, which is sometimes contraindicated in patients with cardiac disease. However, these techniques are used extensively in people, and specific veterinary clinical applications are starting to emerge.
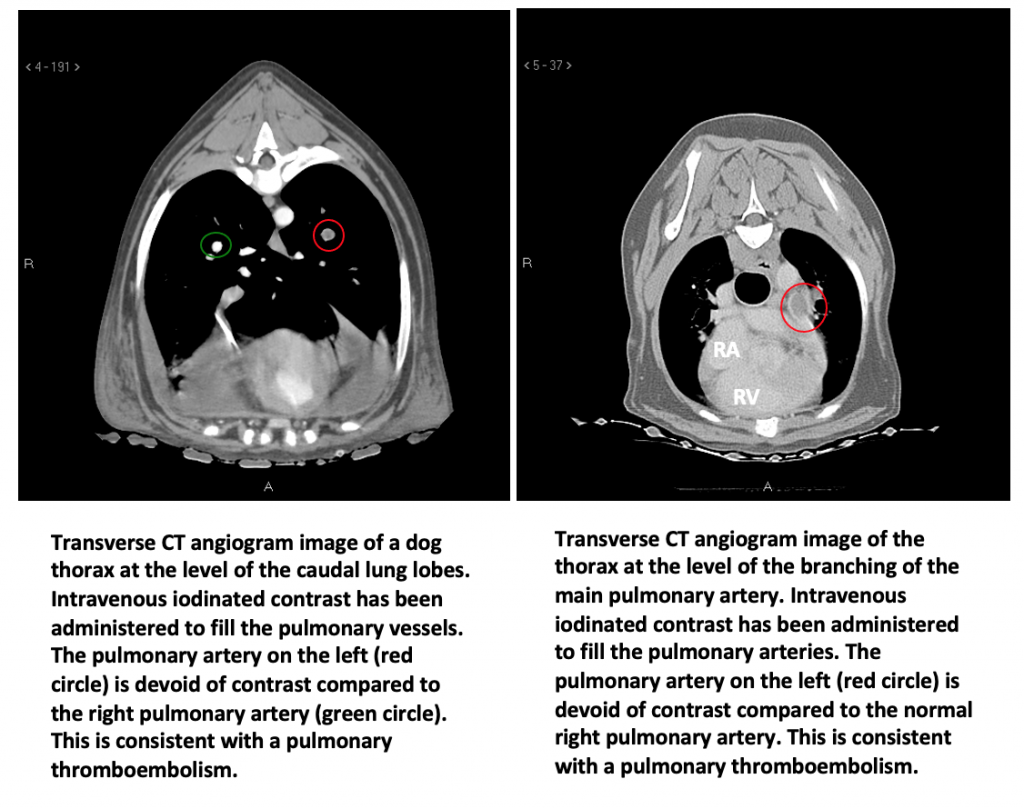
CT is our best modality for evaluating the pulmonary vessels and the presence of thrombi in the pulmonary arteries. Although radiographs allow the visualization of the pulmonary vessels, it is difficult to assess their lumen without the use of CT angiography, cardiac catheterization or MRI. Pulmonary thromboembolism (PTE), which is the occlusion of a pulmonary artery with a blood clot, is a disease that can cause a profound disruption to the perfusion of the lungs and respiratory distress.
REFERENCES / OPTIONAL READING
- Buchanan JW. Vertebral scale system to measure heart size in radiographs. Vet Clin North Am Small Anim Pract. 2000; 30: 379-393, vii.
- Litster AL, Buchanan JW. Vertebral scale system to measure heart size in radiographs of cats. J Am Vet Med Assoc. 2000; 216: 210-214.
- Berry CR, Graham JP, Thrall DE. Interpretation paradigms for the small animal thorax. In: Thrall DE(ed): Textbook of veterinary diagnostic imaging. St. Louis: Saunders, 2007;462-485.
- Moon ML, Keene BW, Lessard P, Lee J. Age related changes in the feline cardiac silhouette. Veterinary Radiology & Ultrasound. 1993;34: 315-320.
- Jepsen-Grant, K., Pollard, R.E., et al. (2012). Vertebral Heart Scores in Eight Dog Breeds. Veterinary Radiology & Ultrasound 54(1): 3-8.