Faculty Syllabus: ECG III: Arrhythmias
ECG III: ARRHYTHMIAS
John E. Rush, DVM, MS, DACVIM (Cardiology), DACVECC
Cummings School of Veterinary Medicine at Tufts University
OBJECTIVES
This section concentrates on ECG interpretation. While therapy is mentioned for your interest, do not try to remember treatment protocols at this stage. Those marked *** are especially important.
1. Be able to determine the heart rate given an ECG recorded at 25 mm/sec or 50 mm/sec.
2. Be able to identify normal sinus rhythm and sinus bradycardia or sinus tachycardia in the dog, cat, horse and cow.
3. Be able to identify sinus arrhythmia and wandering pacemaker and recognize this rhythm as normal in the dog and horse.
4. Be able to identify supraventricular premature depolarizations and supraventricular tachycardia (atrial premature depolarizations and junctional premature depolarizations).
5. Be able to recognize atrial fibrillation, recognize disease associations for this rhythm in cats, dogs, horses and cattle, and outline therapy for these species.
6. Be able to identify ventricular premature depolarizations, ventricular tachycardia and ventricular fibrillation.
7. Be able to identify sinoatrial arrest and differentiate it from atrial standstill. List common causes of atrial standstill.
8. Be able to recognize junctional escape complexes and ventricular escape complexes. Be aware that these complexes are acting as a protective mechanism and result from a failure in impulse formation or conduction.
9. Recognize first degree AV block, second degree AV block and third degree AV block.
CARDIAC DYSRHYTHMIAS: DIAGNOSIS AND TREATMENT
1. INTRODUCTION
A. Abnormalities of cardiac rhythm and conduction are common in veterinary medicine.
1. They may be caused by primary myocardial disease, disease of the conduction system, valvular disease, myocardial ischemia or infarction; or
2. Conditions which secondarily affect the heart, e.g. anemia, acidosis, trauma, shock,
electrolyte disturbance, etc.
B. Their significance is dependent on the type of dysrhythmia (arrhythmia) and the clinical setting in which it occurs. Dysrhythmias must be interpreted with the patient and its problems in mind.
C. Classification – there are a number of ways in which dysrhythmias may be classified, for example: ***
1. Brady or tachyarrhythmias – those which cause slowing or speeding of the heart rate. Some dysrhythmias, however, do not noticeably affect rate.
2. Anatomic origin – e.g. supraventricular vs. ventricular.
3. “Physiologic” vs. pathologic – this is sometimes difficult to determine, therefore, the entire clinical picture must be appreciated.
4. Timing – e.g. premature vs. escape – the time when an ectopic complex occurs with respect to the dominant rhythm.
5. Frequency and distribution – when and how often the dysrhythmia occurs, e.g. bigeminal distribution.
D. Hemodynamic Alterations
1. Dysrhythmias can significantly affect cardiovascular hemodynamics.
a. The clinical significance depends on the previous cardiovascular status, e.g. a dog with compensated mitral insufficiency can decompensate rapidly if atrial fibrillation develops.
2. While variable between patients, healthy dogs can tolerate heart rates ranging from approximately 40-60 to 160-180 bpm without adversely affecting cardiac output. However, diseased patients are less tolerant of rate fluctuations. Tachyarrhythmias alter cardiac output by decreasing ventricular filling time, reducing coronary perfusion and increase myocardial oxygen demand.
3. Atrial and ventricular premature contractions may result in a 25-50% decrease in cerebral circulation.
4. Coronary blood flow may decrease to 60% of normal during uncontrolled atrial fibrillation and 40% of normal during severe ventricular tachycardias. The significance of this decrease partly depends on the previous state of health (or disease) of the myocardium.
5. Renal blood flow may be decreased by 20% during atrial fibrillation and by 60% during ventricular tachycardia.
In the following sections, the dog is the model for “normal vs arrhythmia” unless otherwise noted. Most descriptions are readily applicable to other species, if you take into consideration the normal heart rates and complex intervals for the different species
APPROACH TO ARRHYTHMIA DIAGNOSIS *** useful to have some consistent approach; this is one approach
1. General inspection of the ECG
2. Determine heart rate
a. Normal rate or
b. Bradycardia or
c. Tachycardia
3. P waves for every QRS?
a. Related?
4. QRS for every P wave?
a. Related?
5. Identification of premature complexes
a. Supraventricular or
b. Ventricular
6. Identification of pauses in the rhythm
a. What caused the pause?
b. What ends the pause?
7. Summarize ECG diagnosis
SINUS RHYTHMS *** know all the sinus rhythms
A. Normal rhythms originating in the sinoatrial node
1. Normal sinus rhythm (NSR) – regular impulse formation results in regular P wave formation. If atrial, A-V nodal and ventricular conduction are normal then regular P-QRS-T complexes result.
a. ECG signs:
(1) Normal rate
(2) Regular P-P and R-R intervals
(3) P-QRS-T complex relationship normal (there is a P for each QRS-T and they are related)
b. NSR may be accompanied by abnormal A-V nodal or ventricular conduction or by competing ectopic rhythms. Some of these abnormalities are described below.
REGULAR SINUS RHYTHM
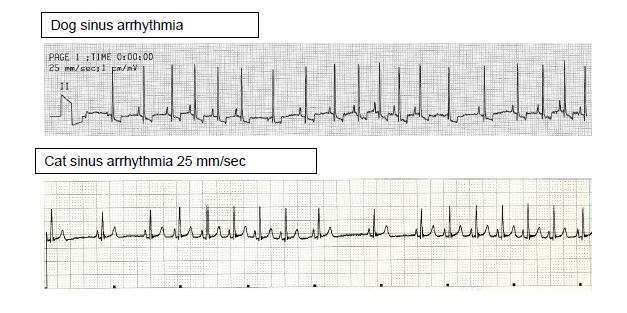
2. Irregular sinus rhythm (sinus “arrhythmia”)
a. Associations – normal, particularly in dog and horse; due to changing vagal tone. May be pronounced with concomitant bradycardia, especially in animals with upper respiratory deformities (redundant palates, tracheal collapse, etc.), cervical masses or brainstem lesions which accentuate vagal tone.
b. ECG signs
(1) Slow to normal rate; occasionally escapes occur if the rate is very slow. In respiratory SA, the HR increases during inspiration.
(2) Cyclic irregularity of rhythm (irregular P-P/R-P)
(3) P-QRS-T complex (normal P-QRS-T relationships exist)
(4) If a “wandering pacemaker” exists, the P wave will regularly and gradually change its configuration as the rate speeds during inspiration and slows during expiration.
c. Treatment – none required
SINUS ARRHYTHMIA
ABNORMAL RHYTHMS ORIGINATING FROM THE SINOATRIAL NODE
1. Sinus bradycardia
a. Associations – excess vagal tone, head trauma, brainstem lesions, increased CSF pressure, “toxemias,” hyperkalemia or other electrolyte disturbances, hypother-mia, drugs (beta-blockers, calcium channel blockers, sedatives)
b. ECG signs
(1) Rate less than 60 (dog), 160 (cat), 46 (Bovine), 24 (Equine)
(2) Regular sinus rhythm or sinus arrhythmia present
(3) P-QRS-T complex usually normal
c. Treatment – none, unless rate drops below 40-50 or animal is symptomatic, then use parasympatholytic (i.e., atropine) or sympathomimetic (i.e., epinephrine). Treat the primary cause.
SINUS BRADYCARDIA

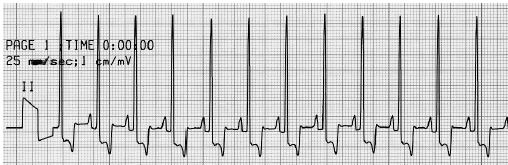
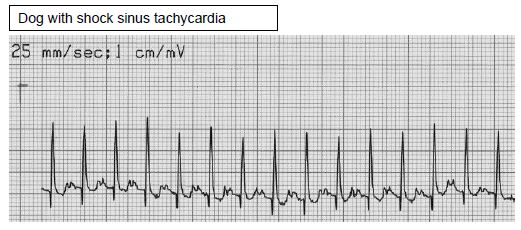
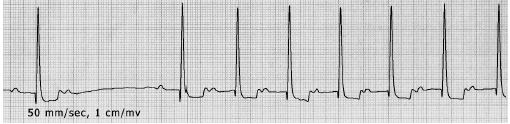
2. Sinus tachycardia
a. Associations – excitement, pain, fear, heart failure, fever, hyperthyroidism, shock and other causes of SNS discharge
b. ECG signs
(1) Rate greater than 160 bpm – toys) (>60 in horses)
(2) Regular rhythm (slight difference in R-R intervals
occasionally)
(3) Normal P-QRS-T complexes (normal P-QRS-T relationship)
(4) P and T waves may superimpose due to rapid rate
c. Treatment – treat primary cause. ß-blockers or digitalis probably would slow sinus rate but are rarely given.
SINUS TACHYCARDIA
PREMATURE DEPOLARIZATIONS AND TACHYARRHYTHMIAS
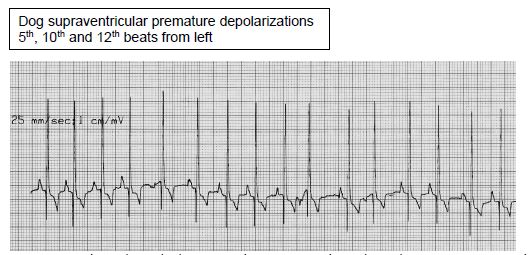
1. Supraventricular premature depolarizations (premature impulses originating the atria or A-V junction) ***
a. Association – chronic valvular or myocardial heart disease, toxemia, digitalis intoxication, atrial stretch, pulmonary disease or pulmonary hypertension.
b. ECG signs
(1) Irregular R-R intervals due to premature impulses
(2) Premature QRS is relatively normal and usually associated with an “ectopic P” wave (which may be “buried” in the previous T wave).
(3) The P-R interval is usually different than normal (altered A-V cond.)
(4) There may or may not be a full compensatory pause. In classical atrial premature depolarizations, the pause is less than compensatory due to premature depolarization and resetting of the sinus node.
(5) One may speculate as to the site of origin of extrasystole by examining the P’ wave and where it occurs with relation to the QRS but often this is tenuous. Correlations suggested for Lead II:
(a) Upright P’ wave before the QRS; Rt. atrial impulse
(b) Negative P’ wave before the QRS with increased PR interval; Lt. atrial impulse
(c) No P’ wave or negative P’ wave just preceding the QRS or buried in the ST-T segment of the QRS; junctional impulse
c. Treatment
(1) Digitalis – particularly if in CHF; remove digitalis if it’s causing arrhythmia
(2) ß blocker
(3) Calcium channel blocker
(4) Infrequent supraventricular premature depolarizations and/or those not associated with clinical signs do not require therapy.
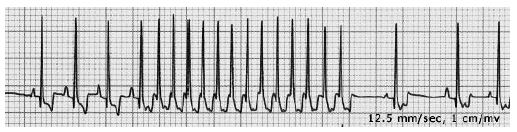
2. Supraventricular tachycardia (Paroxysmal supraventricular tachycardia = PSVT; Paroxysmal atrial or junctional tachycardia = PAT or PJT). ***
a. Associations – any cause of atrial dilatation or disease, atrial or A-V conduction disease or accessory conduction pathways, neoplasia, electrolyte disturbances
b. ECG signs
(1) Rapid heart rate often paroxysmal (i.e. starts and end abruptly)
(2) Fairly regular impulse formation (R-R), although prolongation of atrial-ventricular conduction may result in variable R-R intervals
(3) Ectopic P’ waves may present and related to the QRS via anterograde or retrograde connections. Any P wave configuration is possible.
(4) QRS is typically normal
(5) Mechanisms include:
(a) Ectopic atrial pacemaker that spontaneously discharges (often tachycardia ends with block P’) or reentrant pathways usually involving conduction through different A-V junctional pathways (“longitudinal dissociation”). See below:
c. Treatment options:
(1) Vagal maneuver (carotid or ocular pressure) may disrupt reentry, breaking the SVPT.
(2) Digitalis
(3) ß blocker
(4) Calcium channel blocker
(5) ECG synchronized cardioversion
ATRIAL TACHYCARDIA – PAROXYSMAL
3. Atrial Flutter – a rapid, regular, atrial activation resulting in a rapid atrial rate with physiologic block of some of the impulses in the A-V node causing a slower ventricular response. Can be confused with atrial (supraventricular) tachycardia.
a. Associations – an uncommon rhythm in animals; in horses with atrial fibrillation, the baseline is often so coarse that it appears to be atrial flutter. This rhythm is often “unstable” in animals and either converts back to sinus rhythm or evolves to atrial fibrillation.
b. ECG signs
(1) Rapid or normal rate, depending on degree of physiologic A-V block; rapid atrial rate.
(2) The ventricular response (R-R intervals) is irregular due to a variable degree of A-V block. There is often a relationship between the number of flutter waves and QRSs, e.g. 3:2, 3:1, etc.
(3) The P waves are replaced by ‘saw-toothed’ flutter waves (‘F’ waves).
(4) Absent isoelectric shelf in some leads.
c. Treatment
(1) Digitalis, calcium channel blocker or ß-blocker may slow the ventricular rate by delaying A-V nodal conduction. Cardioversion can be done
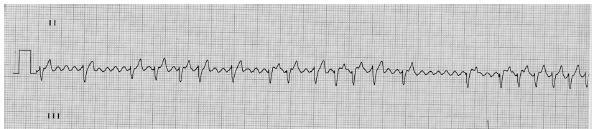
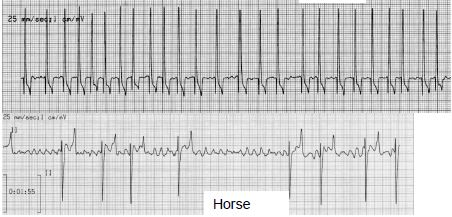
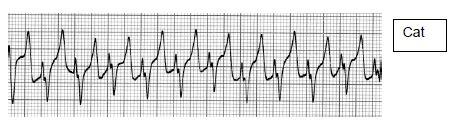
4. Atrial Fibrillation (AF) ***
a. Associations – cardiomyopathies of giant breeds (St. Bernard, Great Danes, etc.), chronic mitral valve disease, congenital heart diseases; sometimes spontaneously in horses and cattle.
b. ECG signs
(1) Rapid rate, irregular ventricular rhythm (irregular R-R intervals)
(2) No P waves
(3) Fibrillation (‘F’) waves (baseline undulations) are usually present.
(4) QRS appears normal although slight differences between the complexes due to variable A-V conduction are common.
c. Treatment
(1) Quinidine or cardioversion are not generally successful in obtaining permanent conversion, except in the horse and cow. Spontaneous conversion is very common in large animals.
(2) Oral quinidine is given to horses to convert AF to NSR.
(3) Cattle usually convert spontaneously to NSR.
(4) Digitalis, ß-blockers or calcium channel blockers to slow the ventricular response by reducing the number of impulses reaching the ventricles.
(5) In most dogs and cats, conversion from AF to NSR does not occur and treatment is directed at reducing the number of impulses reaching the ventricle by slowing A-V conduction and, accordingly, ventricular rate, to improve cardiac filling and increase cardiac output.
ATRIAL FIBRILLATION
5. Ventricular Premature Depolarizations aka Ventricular Premature Contractions aka Ventricular Premature Complexes aka Ventricular Extrasystoles = VPC, VPD, Premature Ventricular Depolarization – PVD, Premature Ventricular Complex – PVC ***
a. Associations – Numerous
(1) Primary myocardial disease including tissue hypoxia or ischemia due to heart failure, microscopic intramural myocardial infarction (MIMI), cardiomyopathy, bacterial or toxic endomyocarditis, traumatic myocarditis, neoplasms, etc.
(2) Extracardiac diseases causing myocarditis or ischemia such as pyometra, sepsis, gastric dilatation, uremia, head trauma, pancreatitis, acidosis, hypoxia due to pulmonary disease, “autonomic imbalance”, etc.
(3) Electrolyte imbalances, particularly hypokalemia.
(4) Drug induced VPDs including digitalis, epinephrine, halothane, etc.
b. Nomenclature – distributional pattern
(1) Single – 1 VPC
(2) Doublet – 2 VPCs
(3) Run – 3 VPCs
(4) Tachycardia – 3 or more (usually more) VPCs linked together
(5) Bigeminy – every other QRS is ectopic
(6) Trigeminy – every 3rd QRS is normal or ectopic (2 variants)
c. ECG signs (see Figures)
(1) The ectopic complex breaks the normal rhythm by occurring early (premature – extrasystole).
(2) The ectopic beat may (or might not) appear “coupled” to the preceding normal P-QRS-T.
(3) A compensatory pause usually follows an isolated VPC.
(4) The QRS is widened and bizarre when compared with a normally conducted QRS and the T wave is widened and oriented in a direction opposite to that of the ectopic QRS. The isoelectric shelf in the ST segment is frequently absent.
(5) If the ectopic QRS originates from the right ventricle, the QRS complex resembles those seen in left bundle branch block (upright and widened in lead II). If the ectopic QRS originates from the left ventricle, the QRS usually looks like those seen with right bundle branch block (negative and widened in lead II).
(6) If the extrasystole occurs late in diastole (after P wave) but before the sinus impulse completely depolarizes the ventricles, a fusion complex results.
(7) If the ventricular extrasystoles vary in QRS morphology, this may indicate that there is more than one ectopic focus and the extrasystoles are therefore multifocal.

6. Accelerated ventricular rhythm (idioventricular tachycardia) – in this dysrhythmia a regular ectopic ventricular rhythm temporarily assumes control of the heart at a rate that is close to that of the basic sinus rhythm. The rate of impulse formation of the ectopic focus is slower than that “typically” associated with ventricular tachycardia. Fusion beats are frequently noted. Accelerated ventricular rhythm is often a “race” between the sinus node and the ectopic focus. When the sinus node slows, the ventricular focus depolarizes the ventricles.
a. Associations – similar to those of ventricular extrasystoles; very common with digitalis intoxication, gastric torsion, autonomic imbalance.
b. ECG signs
(1) The rate is variable, but usually greater than 60/min and
less than 160/min (dog).
c. Can be thought of as a “slow” ventricular tachycardia.
Accelerated ventricular rhythm (note fusion = F)

7. Ventricular tachycardia – More than three successive ventricular extrasystoles occur at a rapid rate (usually significantly faster than the sinus rate and usually above 160 beats per minute in dogs and cats).
a. Associations – same as ventricular extrasystoles
b. ECG signs
(1) A ventricular pacemaker fires at a rapid rate resulting in a series (greater than 3) of linked ventricular ectopic impulses.
(2) P waves may be noted to be “buried” in the QRS-T complexes, but this atrial rate is slower than the ventricular rate and the P waves are not conducted.
(3) Following spontaneous conversion, a normal rhythm with normal P-QRS-Ts may ensue, or ventricular singles, pairs, runs or tachycardia may quickly follow.
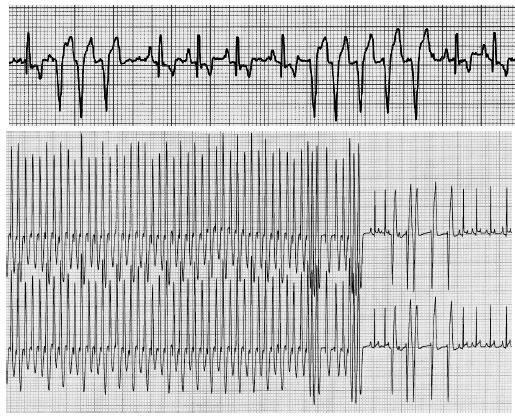
8. Ventricular Fibrillation *** – is an irregular and disorganized ventricular activity incompatible with life and characterized by a lack of recognizable QRS-T complexes. It may be preceded by ventricular flutter which is a ventricular rhythm that appears like a sine wave with no clear QRS or T wave.
VENTRICULAR FLUTTER DEGENERATES INTO VENTRICULAR FIBRILLATION

VENTRICULAR FIBRILLATION

9. Recognition, Significance and Treatment of Ventricular Extrasystoles, Parasystoles, Accelerated Rhythms and Tachycardia
a. Anatomic origin
(1) Multifocal ventricular discharges are generally more serious than unifocal ectopia in an identical clinical setting as they likely indicate more widespread disease in the ventricle.
b. Time of appearance
(1) The ventricle is hyperexcitable during repolarization and if stimulated, may fibrillate. This roughly corresponds to the “T” wave on the ECG. For this reason, premature impulses occurring on the T waves are more dangerous than premature impulses occurring after the T waves.
(2) Late diastolic VPDs impair hemodynamics less than early diastolic VPDs since there is added time for ventricular filling.
c. Rate of ectopic rhythm – in dogs, ventricular tachycardias become “serious” if their rate exceeds 160-180 bpm.
d. Frequency of extrasystoles
(1) Occasional VPCs are common in diseased or even apparently healthy animals. Some of these may be precipitated by fear or excitement, some are due to anesthetics, drugs and some are idiopathic. When infrequent VPCs are not due to serious organic diseases they can probably go untreated.
e. Therapeutic approach to ventricular dysrhythmias. The arrhythmia should be treated in light of knowledge of the underlying disease, electrolyte and blood gas status, and severity of the arrhythmia. Some ventricular arrhythmias do not require treatment. Others are treated with a variety of drugs including Lidocaine, Procainamide, Quinidine, ß-blockers like propranolol, and a variety of other drugs.
FAILURE OF IMPULSE FORMATION
1. Sinoatrial arrest ***
a. Associations – causes of increased vagal tone; brachycephalic breeds with respiratory deformities and vagovagal reflexes; sinus node disease (“sick sinus” syndrome) – reported in middle aged to older miniature Schnauzers, Pugs, Dalmatians and other breeds. These animals often present for syncope. Prognosis is good for longevity but recurrent syncope is common.
b. ECG signs
(1) Slow or normal rate
(2) Pauses equal to (SA block) or greater than (SA arrest) two P-P intervals without demonstrable atrial activity (no P waves). First determine the normal P-P interval, esp. in dogs with sinus arrhythmia.
(3) P-QRS-T complexes predominate but junctional and ventricular escapes are common.
(4) May be associated with sinus arrhythmia or wandering pacemaker
(5) In classic “sick sinus” pronounced sinus bradycardia alternates with periods of sinus or supraventricular tachycardia.
c. Treatment – pacemaker best if symptomatic (syncope); occasionally atropine or propantheline is effective.

2. Atrial Standstill (Hyperkalemia) ***
a. Associations – hyperkalemia due to Addison’s disease, urinary obstruction, renal failure, acidosis.
b. Definition – atrial standstill refers to the absence of P waves noted in hyperkalemic patients. The atria lose their ability to become excited and thus a P wave cannot be generated. The SA node is highly resistant to hyperkalemia, and the rhythm may be sino-ventricular, i.e. originating in the SA node, spreading through specialized internodal pathways to the A-V node, and then to the ventricles. Since hyperkal-emia affects both the depolarization (prolongs) and repolarization (shortens) phases of ventricular tissue, changes in both the QRS and T wave are seen. These are somewhat dependent on serum calcium, acid-base status and sodium concentration. Eventually ventricular depolarization and repolarization become “intertwined” resulting in a sine-wave like QRS-T.
c. ECG signs
(1) Initially, sinus tachycardia (reduced resting potential)
(2) Later, bradycardia (effect on K+ ion drift across cell membrane)
(3) Flattening, then loss of the P waves
(4) Gradual changes in the ST-T segment (depression or elevation)
(5) Tented or peaked T waves (shortened repolarization)
(6) Widening of the QRS (prolonged depolarization and fascicular blocks)
(7) QRS and T wave fusion (“sine-wave” QRS-T)
d. Treatment – always treat the primary disease in addition to the hyperkalemia. Sodium bicarbonate, calcium gluconate and insulin with dextrose may be helpful in correcting hyperkalemia.
HYPERKALEMIA IN A DOG AND A CAT – 25 MM/SEC

3. Persistent atrial standstill – a rare disorder in dogs (Springer Spaniels predisposed) characterized by persistent absence of P waves associated with atrial muscular dystrophy and loss of atrial myocytes – often the ventricular myocytes are eventually affected.
RHYTHMS RESULTING FROM FAILURE IN IMPULSE FORMATION OR CONDUCTION
A. Junctional escape complexes ***
1. Associations – single junctional escape complexes result from an interruption in normal sinus node impulse formation (e.g. sinus bradycardia, sinus arrest) or impulse conduction (e.g. SA block, A-V block). Escapes are protective mechanisms that ensure electrical-mechanical functions will continue. Escape complexes are always secondary to ECG diagnosis since they are predicated on a primary rhythm disturbance, i.e. sinoatrial arrest with junctional escape complexes.
2. ECG signs of junctional escapes
a. Heart rate usually slow.
b. Irregular R-R intervals indicate irregular impulse formation or conduction.
c. Junctional originated QRS complexes follow pauses “rescuing” the ventricle by providing a focus of impulse formation.
d. Normal P-QRS relationship not present.
e. P waves, if present, are usually negative in Lead II (retrograde) and can precede, follow or be buried in the QRS. The P wave is dependent on the location of the ectopic focus and anterograde and retrograde impulse conduction.
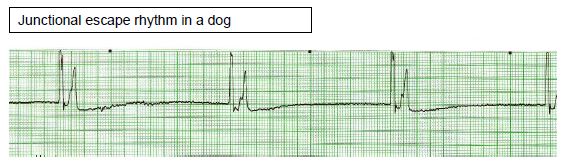
B. Junctional escape rhythm (“idionodal rhythm,” “passive junctional rhythm”)
1. Associations – multiple junctional escape complexes occur in sequence as a result of abnormal impulse formation in the SA node (e.g. sinoatrial arrest, sinus bradycardia) or delayed conduction through the A-V node (e.g. 2 or 3 A-V block). They are protective mechanisms for the heart and result in slow regular rhythms at the inherent discharge rate of the normally suppressed junctional pacemaker cells. If the sinus mechanism is permanently absent, a continual junctional rhythm occurs. In those cases where junctional pacemakers depolarized at a rapid rate junctional tachycardia or accelerated junctional rhythm are better terms to use.
2. ECG signs of junctional escape rhythm
a. The heart rate is generally slow (50-70/minute)
The R-R interval is usually regular although “warming-up” causes the R-R intervals to shorten slightly as the rhythm is established.
c. Retrograde P waves (negative in leads II and aVF) may be noted following the QRS.
d. The QRS is usually oriented normally.
3. Treatment – never suppress escape rhythm. Treat primary rhythm abnormally (e.g. junctional escape rhythm in A-V block) (escape focus below block).
C. Ventricular escapes *** – single or multiple ectopic ventricular depolarization that follow the preceding QRS by an interval longer than the predominant R-R interval. Escapes are not premature. They occur as a compensatory response to failure of normal supraventricular activation of the ventricles. If the higher pacemaker focus fails to discharge or its impulse is blocked for an extended period, the ventricular escape focus may initiate a slow stable rhythm at its own (slow) inherent rate. This occurs in complete A-V block. The ventricular rhythm is termed slow ventricular rhythm or Idioventricular rhythm (see below).
1. Associations – supraventricular bradycardias such as sinus bradycardia, sinoatrial arrest; conduction disturbances such as the A-V blocks
2. ECG signs
a. Ectopic depolarizations occur late, after the dominant pacemaker should have discharged and depolarized the ventricles.
b. There may or may not be a preceding P wave, however, if present, the P wave is not conducted to the ventricle.
c. The QRS is widened and bizarre, being ventricular in origin. The T wave is wide and oriented opposite the QRS.
d. The ventricular focus will discharge slowly (usually 28-40/minute) and regularly at its own inherent rate causing an idioventricular rhythm. A brief “warm up” period may occur as the ectopic pacemaker establishes its inherent rate.
3. Treatment – never treat or suppress an escape rhythm; they are protective mecha-nisms! One does not make a primary diagnosis of “escape complexes.” The abnormality which leads to ventricular escapes must be defined.
DISTURBANCES OF ATRIOVENTRICULAR CONDUCTION
1. First degree (1 degree) atrioventricular (AV) block – conduction is delayed through the A-V node causing lengthening of the PR interval. ***
a. Associations – due to high vagal tone is often a physiologic dysrhythmia in horses and some dogs. Digitalis, some antiarrhythmic drugs (digitalis) and sedatives (xylazine) cause this rhythm.
b. ECG signs
(1) The rate is variable.
(2) There is a P wave for each QRS-T and vice versa
(3) The P-R interval is prolonged.
(4) Occasionally the P-R interval varies.
15
(5) 2nd degree A-V block may also be present.
c. Treatment – not necessary, however, if drugs are causing this rhythm their use should be reevaluated.
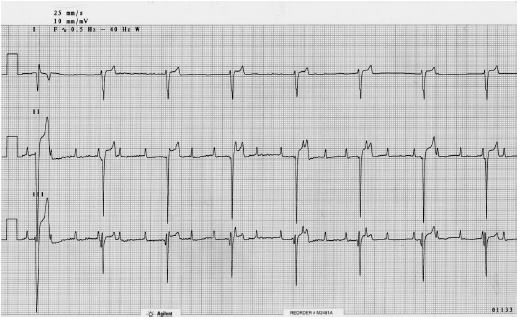
FIRST AND SECOND DEGREE AV BLOCK IN A DOG
2. Second degree (2 degree) Atrioventricular (AV) block – in second degree AV block, some atrial impulses are blocked or nonconducted, thus some P waves are not followed by a QRS-T. Some ventricular beats are “dropped.” ***
(a) Mobitz type I (Wenkebach) – the PR interval gradually prolongs until a ventricular beat is dropped (i.e., a QRS does not follow a P wave).
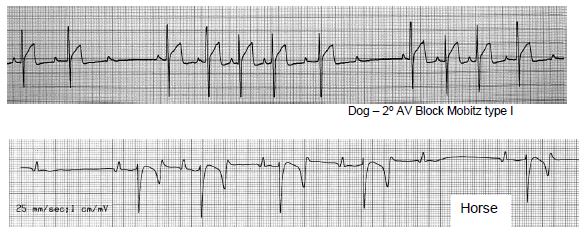
(b) Mobitz type II – the PR intervals are constant, however, some P waves are not followed by a QRS.

a. Associations – Mobitz type I block often is associated with block high in the A-V node. It is a normal phenomenon in resting horses. Mobitz type II block is a moreadvanced degree of block, usually occurs in the A-V junction or His bundle, and it often indicates disease in the conduction system or an electrolyte abnormality.
b. ECG signs
(1) The rate is usually slow
(2) Some P waves not followed by QRS-Ts (blocked at AV node).
(3) In Mobitz type I block, the PR interval prolongs until a P wave is not followed by a QRS-T.
(4) In Mobitz type II block, the PR interval is constant; however, some P waves are not followed by a QRS-T.
(5) Escapes, either junctional or ventricular, noted after pauses.
c. Treatment – in some cases, anticholinergic drugs abolish vagal influence and result in normal sinus rhythm. Other sympathomimetic drugs may speed A-V conduction and abolish the block. In most cases, treatment is not necessary. Electrolyte status should be evaluated and offending drugs removed if indicated.
3. Third degree (3) Atrioventricular (AV) block – aka “complete heart block” – there is an anatomic or persistent physiologic interruption in impulse conduction through the A-V node. No P waves are conducted through to the ventricle, and the dominant rhythm is supplied by a focus located below the block in the AV junction or ventricle. ***
a. Associations – disease of the conduction system: infarcts, infection, neoplasms, granulomas, degeneration or hemorrhage in the A-V node; in dogs – idiopathic atrophy of A-V nodal tissue with replacement with connective tissue, fat or cartilage is frequently reported as the cause of complete A-V block in older dogs and cats.
b. ECG signs
(1) The heart rate is slow (usually less than 50/minute)
(2) There are more P waves than QRS-Ts.
(3) There is no consistent relationship between the P waves and the QRS-T. No P waves are conducted to the ventricle.
(4) The QRSs are the result of pacemaker activity below the level of the A-V block. Sometimes the dominant pacemaker is idionodal. Sometimes the pacemaker is idioventricular.
(5) The administration of drugs (parasympatholytics or sympathomimetics) does not cause P waves to be conducted through the A-V node if there is anatomic disruption.
c. Treatment – There is no effective medical therapy. In emergency situations, the junctional or ventricular escape rate can be increased with sympathomimetic drugs. Treatment of choice is an implantable pacemaker.
THIRD DEGREE AV BLOCK AND A JUNCTIONAL ESCAPE RHYTHM

THIRD DEGREE AV BLOCK AND A VENTRICULAR ESCAPE RHYTHM
VENTRICULAR PRE-EXCITATION.
In pre-excitation the conduction from atria to ventricles is accelerated due to accessory A-V pathways. This results in a short P-Q interval. These are rare in animals.
A. Wolfe-Parkinson-White (WPW) – partial pre-excitation of the ventricle via an anomalous A-V bridge (Kent bundle) causes part of the ventricle to be depolarized before the normal impulse is through the A-V junction. ECG signs include: short P-R, slurred initial QRS (delta wave), widened QRS and PSVT via reentry through anomalous pathway.
B. Short P-R, syndrome [Lown-Ganong-Levine (L-G-L)] – complete pre-excitation of the ventricles via the A-V nodal bypass tract (James bundle or Mahaim fibers) resulting in a short P-R, normal QRS and PSVT via reentry.

ABNORMALITIES OF REPOLARIZATION (ST-T CHANGES)
A. The ST segment and the T wave (the ST-T segment) represent ventricular repolarization.
1. Changes in repolarization can be due to a number of factors including: primary myocardial disease, altered activation of the ventricle as noted with ventricular enlargement or abnormal conduction such as right bundle branch block, hypoxia, ischemia, electrolyte abnormalities, and many other factors.
B. Primary T wave changes are often non-specific.
1. The ST-T segment may be elevated or depressed.
2. The ST segment may slur or cove into the T wave (ST segment coving).
3. The repolarization process may be shortened or lengthened resulting in tall peaked T waves or prolonged T wave (i.e., QT interval shortened or lengthened).
C. Some common associations with altered ST-T segments include:
1. Left ventricular hypertrophy – T wave inversion, ST segment coving
2. Endocardial or epicardial injury current-elevation/depression of ST
3. Pericardial disease – ST-T elevation and possible electrical alternation of the QRS and/or ST-T segment (big then small)
4. Electrolyte abnormalities, particularly calcium and potassium
a. Low calcium lengthens/high calcium shortens the QT interval.
b. High potassium – shortens the repolarization process causing peaked and tented T waves.
c. Low potassium – may cause U waves after the T wave (uncommon and difficult to recognize).
5. Hypoxia – ST segment depression or elevation
6. Digitalis – non-specific ST changes or J point depression in the dog.
7. Exercise – causes physiologic T wave changes particularly in the equine where it can cause T waves to flip from positive to negative.
ST SEGMENT DEPRESSION IN A DOG