Insomnia is the most common sleep disorder, and approximately 30% of adults experience symptoms of insomnia worldwide. There is a 10% prevalence of daytime impairment and distress as a result of insomnia, and a 6% prevalence of insomnia symptoms that persist for at least one month without the presence of another disorder, medical condition, or substance. There are many risk factors for insomnia such as age and gender, with older adults and women being more susceptible. Comorbid medical disorders, psychiatric disorders, and working night shifts are also risk factors. Insomnia also results in increased risk for comorbid medical disorders such as neurodegenerative disorders or other psychiatric disorders. In general, chronic insomnia is associated with substantial decreases in quality of life (1).
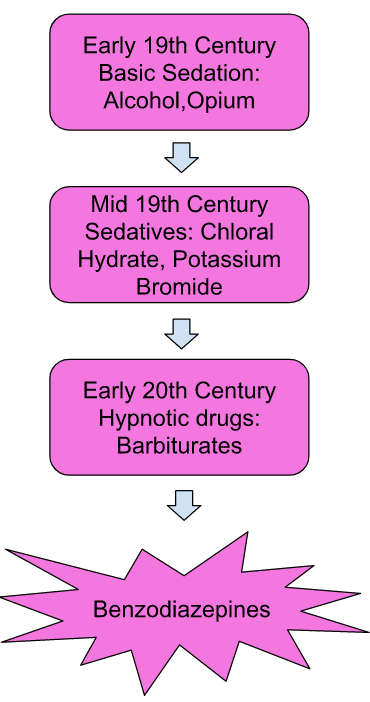
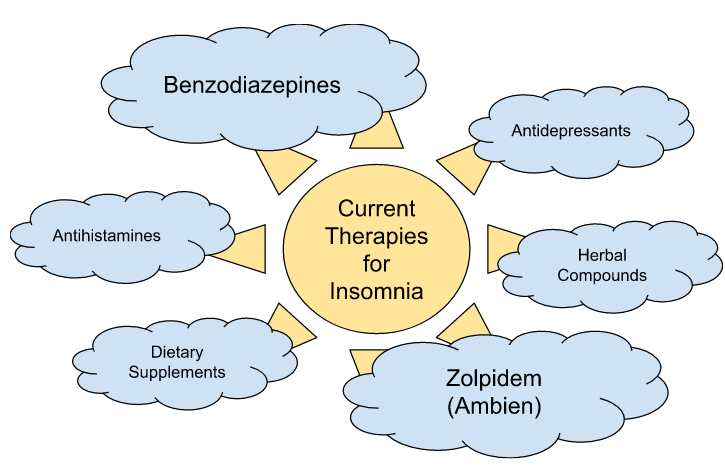
As shown in Figure 1, the development of modern sleep medicine started with the use of common sedatives and evolved into the creation of a class of sedative drugs called benzodiazepines. Benzodiazepines such as chlordiazepoxide and diazepam became favored due to their low toxicity and sedative potency, and they remain as the one of the few formally approved insomnia drug treatments in the US (2). As the 21st century continued, additional non-benzodiazepine drugs were approved by the FDA for use. Chief among them is zolpidem, widely known as Ambien. In addition to these drugs, several other therapies for targeting insomnia have developed from non-sedative drugs. These therapies are detailed in Figure 2. While these alternative therapies have been used with the primary purpose of treating insomnia, that use is either unregulated or unapproved by the FDA. Treatments based on cognitive and behavioral therapies are also used as alternatives to drug treatment (2).
Although current understanding of the mechanisms of sleep and the causes of insomnia are still constantly evolving, and the mechanisms of action of sedative hypnotic drugs are still being studied, significant progress has been made over the last few decades in understanding how to treat sleep disorders and how current drug treatments work.
I think this section did a great job on further enhancing on why insomnia matter and why study and learning about how insomnia/mechanism of sleep matter. However, I think it is a bit too dense for the question section. I believe a brief background and key point of why insomnia matter (what is already in the question section) are already enough to make me interested in the topic. The addition of this section, especially the first paragraph, feels like list-making number of reason on why insomnia matter. I would recommend organize some key information here and combine with the question section.
We initially had one “Question” section but split it into two pages so we could preview some treatments for insomnia and the evolution of treatments over time. The goal was to lead into the answer section where we discuss the mechanisms of these drugs (which is also why the drugs are not explicitly defined yet).
I think for the first paragraph that you should use citations and include how the authors acquired the data. It does’t have to be in depth but I know I always question random statistics. I would also change the opening line to take out the “In figure 1,” and word it such that it is included at the end of the sentence as (Figure 1). Have you looked into anything on the negative effects of these drugs you talk about too? (this is without reading the rest of the website)
It may just be me, but it might be beneficial to define “prevalence”. I forgot what it meant and had to look it up (on me).
A small note, I think the figure numbers are supposed to continue from the previous page, so the figure “1” here should be figure “2” and so on. I also agree with Robert to change the reference to the figure as (figure #) after the point is made.
Without having read the rest of the website yet, I don’t know what benzodiazepines are. I also think it could be beneficial to add which symptoms are trying to be addressed by these treatments. Because this is a general background page, a mention may suffice.
in response to monali’s comment. maybe you could provide a link to more information regarding benzodiazepines and drugs, or link them to pages in your website to provide ease of access to information.
We wanted to restart the figure numbering for every page just to keep it consistent (because we only refer to figures on the same page).
To your and robert’s comment about the drugs: again, we are only briefly mentioning the drugs to elaborate on them later in the answer