Whether you are preparing a literature review for your thesis, a journal article, or grant application here are a few tips to help you get started and stay organized:
Determine what information you need.
Why are you searching the literature? Are you developing a research project and want to know what has been published about your topic? Are you interested in literature on a particular method? Are you preparing a grant application or manuscript to submit to a journal? The answers to these questions will help you decide where to search, and whether or not the information that you find is what you need.
Develop a focused question.
If you enter a few words, or a phrase, into a database, then you are likely to retrieve either a very large or very small number of results. Developing a focused research question helps you construct a search strategy that will retrieve a precise set of results. If you have a complex topic, then you may have multiple questions (and searches).
Choose your resources.
Once you have determined what information you need and developed a focused question, then you are ready to choose your resources. Choosing which resources to search can be overwhelming. While PubMed is often a good place to start, think about where, and by whom, information about your topic is likely to be published, and what type of information you need (e.g. journal articles, conference proceedings, patents). What disciplines might have a perspective on your topic? What organizations, associations, institutes, companies or agencies investigate issues related to your topic?
Bibliographic databases, such as PubMed and Web of Science Core Collection, are organized collections of references to published literature (e.g. journal articles, conference abstracts, books). When you are deciding which database(s) to search, consider the subjects, dates, and types of literature the database covers, as well as the search platform. For example, MEDLINE, the database that is the principal component of PubMed, is also available through the Ovid search platform. While PubMed and Ovid MEDLINE are similar, small differences in the content and search features of these two databases means that you will retrieve different results. See the Sackler School Biomedical Sciences Research Guide for a list of biomedical database, or ask me!
Create personal accounts.
You may think that you are finally ready to start searching. Not quite. Create a personal account with the databases, or platforms (e.g. Ovid, Web of Science), that you plan to search. A personal account allows you to save searches and sets of results, and receive email notifications when new results matching your search criteria become available. Unfortunately, you have to create a separate accounts for each database or platform, but it is a good idea to do so for the resources that you use frequently. At the very least, I suggest that you create a My NCBI account, which is the personal account associated with PubMed and other National Center for Biotechnology Information (NCBI) databases, such as Gene and Protein. See the March 2016, May 2016, summer 2016 and December 2016 PubMed Tip of the Month posts for more information on creating and using a My NCBI account.
Use a citation manager.
Choose a citation manager before you embark on a literature review. Citation managers allow you to organize and store your own collection of references, and insert formatted citations and bibliographies into documents. Contact me (laura.pavlech@tufts.edu) if you need assistance selecting or using a citation manager.
Document your search methods.
Get into the habit of documenting the parameters of your search, including: the databases that you searched; the platform on which you searched (e.g. Ovid, Web of Science, etc.); years covered by the database; complete search strategies; any limits applied, such as year, age, language; and the date on which you ran the searches. While this information is not typically required for a manuscript (unless, of course, you are doing a systematic review, meta-analysis or scoping review), or grant application, a literature search is part of your research and should be recorded as you would any other experiment. Doing so saves you considerable time and effort if you need to replicate the search in the future.
If you have limited information about a journal article (e.g. author name and year of publication), then PubMed’s Single Citation Matcher may help you locate the article. Accessible from the PubMed homepage, this tool does exactly what its name implies: it matches citation information to PubMed records. Single Citation Matcher can quickly narrow your search to records that match the information you have.
In a remarkable display of bipartisanship, the Senate passed HR 34 and President Obama signed the 21st Century Cures Act into law on Dec. 13, 2016. The original bill was introduced and sponsored by Rep. Suzanne Bonamici (D-OR) on Jan 2015 and garnered co-sponsors from both sides of the aisle, including the support of Rep. Lamar Smith (R-TX), Chairman of the House Committee on Space, Science and Technology. The House approved the original bill in Oct 2015 and after a year on the Senate floor where the bill underwent several amendments proposed by both Democrats and Republicans, the Senate approved the bill on Dec 6 2016 and passed the bill on to President Obama to be signed into law.
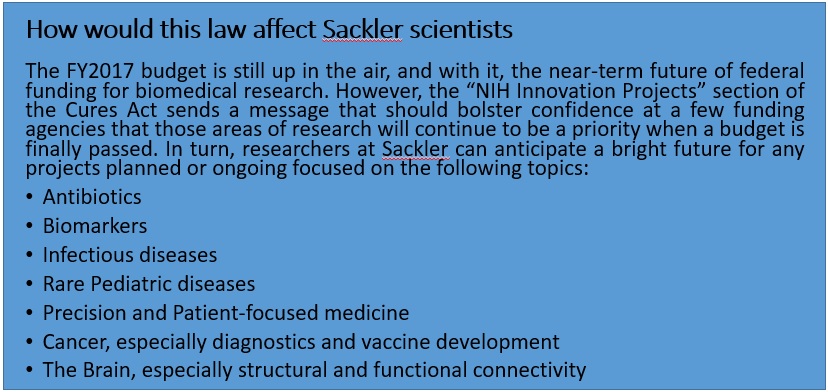
This law is meant to accelerate drug development and bring cutting edge treatment to patients, revise the current status of mental health research and treatment for disorders, with a strong focus on the current opioid crisis sweeping across the nation. The law is also of significant importance to biomedical scientists as it will expand funding for certain fields, keeping in line with the Precision Medicine Initiative launched in 2015. More specifically, the Cures act will provide funding for specific NIH innovation projects such as the Precision Medicine Initiative ($4.5 billion through FY 2026), the BRAIN initiative ($1.51 billion through FY 2026), the Cancer Moonshot project ($1.8 billion through FY 2023) and the Regenerative Medicine (stem cells) program (30$ mn through FY 2026). In addition, this law will stimulate innovative research by awarding investigators with the Eureka Prize for “significant advances” or “improving health outcomes”. The law also seeks to promote new researchers through its Next Generation of Researchers Initiative, an attempt to solve the postdoc crisis in academia. As a response to the lack of women and underrepresented minorities in STEM fields, the law also contains provisions that will attract and retain such scientists in “priority research areas”. Finally, to further encourage early-stage researchers, the law authorizes the establishment of programs to help in the repayment of student loans and raises the cap on the repayment assistance available to the researchers.
Besides ensuring funding for biomedical research, this law aims to address privacy concerns brought up by experts regarding patient information in the era of precision medicine (for more details, check out our analysis of the precision medicine initiative). Under this law, certificates of confidentiality will be provided to all NIH-funded researchers whose studies involve collection of sensitive patient information. This information will be withheld by the NIH, but can be accessed upon requests filed under the Freedom of Information Act. On the other hand, in order to make sure data sharing is made easier for scientists, this law will allow NIH to break out of red tape and regulations that obstruct scientists from attending scientific meetings and sharing data.
Despite the generally positive reception of the Cures Act by NIH officials and research scientists, the bill was not without its critics. The principal criticism of the final product is that it constitutes a handout to pharmaceutical and medical device companies by substantially weakening the FDA’s regulatory check on bringing new treatments into the clinic.
For example, Sydney Lupkin and Steven Findlay point to the$192 million worth of lobbying collectively expended by over a hundred pharmaceutical, medical device, and biotech companies on this and related pieces of legislation. The goal of this lobbying, Lupkin and Findlay assert, was to give the FDA “more discretion” in deciding how new drugs and other treatments gain approval for clinical use – presumably saving a great deal of money for the companies that develop them. Adding weight to their assertion is the fact that President Trump isreportedly considering venture capitalist Jim O’Neill for FDA commissioner. Mr. O’Neill isstrongly supported by libertarian conservatives who see FDA regulations as inordinately expensive and cumbersome, so it seems reasonable to worry about how Mr. O’Neill would weigh safety against profit in applying his “discretion” as head of the FDA. On the other hand, under a wise and appropriately cautious commissioner with a healthy respect for scientific evidence, we might hope that maintaining high safety standards and reducing thecurrent staggering cost of drug development are not mutually exclusive.
Additionally, Dr. David Gorskiwrites of one provision of the Cures Act that appears to specifically benefit a stem-cell entrepreneur whoinvested significantly in a lobbying firm pushing for looser approval standards at the FDA. Once again, it is not unreasonable to suspect that there is room to reduce cost and bureaucratic red tape without adversely impacting safety. And in fairness to the eventual nominee for FDA commissioners, previous commissionershave not been universally praised for their alacrity in getting promising treatments approved efficiently… at least, not within the financial sector. Still, the concerns expressed by medical professionals and regulatory experts over the FDA’s continued intellectual autonomy and ability to uphold rigorous safety standards are quite understandable, given the new administration’senthusiasm for deregulation.
It appears that this law will also allow pharmaceutical companies to promote off-label use of their products to insurance companies without holding clinical trials. Additionally, pharma companies can utilize “data summaries” instead of detailed clinical trial data for using products for “new avenues”. It is possible that these provisions were created with the NIH basket trials in mind (details here). However, as Dr. Gorski argues, without clinical trial data, off label use of drugs will be based on “uncontrolled observational studies”, which, while beneficial for pharma companies, are risky for patients from the perspective of patient advocacy groups. These fears are not without evidence – a recent article from STAT describes how the off-label use of Lupron, a sex hormone suppressor used to treat endometriosis in women and prostate cancer in men, is resulting in a diverse array of health problems in 20-year olds who received the drug in their puberty.
Another “Easter egg”, albeit unpleasant, awaits scientists and policy-makers alike. Buried in Title V of the law is a $3.5 bn cut on Human and Health Services’ Prevention and Public Health fund, without a proper explanation added to such an act. Given the outcry on the lack of public health initiatives in the Precision Medicine Initiative, one is again left to wonder why 21st century cures are focusing only on treatment and drug development and not on policies directed towards promoting public health and prevention of diseases.
In conclusion, the implementation of this law will largely depend on the current administration. With the NIH budget for FY2017 still up in the air, the confirmation of nominees still hanging in balance, this law is far from being implemented. Based on the provisions, it appears that overall biomedical funding will be boosted in particular fields, designated “priority research areas”. However, it shouldn’t fail an observant reader that this bill also seems to allow pharma companies a higher chance to exploit the consumers. It, therefore, still remains a question of whose priorities (consumers/patients vs. investors/corporations) are being put forward first and the answer, in our humble opinion, will be determined by a dialogue between the people and the government.
This month I present, for your reading pleasure, excerpts from my interview with Nafis Hasan from CMDB. Nafis and I had a remarkably wide-ranging conversation covering existential philosophy, cultural differences between Bangladesh and the US, the exquisite symmetry between ecology and cell biology, and current controversies in carcinogenesis research. I can only hope to capture in the space below a mere whisper of his deeply-considered intellectual convictions and passion for social justice. Fortunately, Nafis has also authored an editorial on Science Activism in this very issue, and I strongly urge you, dear reader, to check that out next!
Having a grand time in Dhaka
AH: Where did you grow up?
NH: I grew up in the house that my father and his brothers built in Dhaka, Bangladesh, and moved to the U.S. when I was 18. Most of my dad’s siblings and their families lived with us in Dhaka. As kids, we didn’t really have the notion of “privacy” for the longest time: the elders would each get a room and the kids would sleep in the living room on a big mattress. My cousins and I would all get into trouble at the same time… it was fun!
On the road with college friends
AH: Have you had any opportunities to travel around the States?
NH: For F1 visa (student visa) holders, you have a 3-month window where you have to find a job or get into school. After graduating from Lafayette College [in Easton, Pennsylvania], I thought, “If I have to leave the country, I might as well see it.” So when one of my friends said, “Let’s do a road trip,” I said “Let’s do it!” We started from Pennsylvania, went down to Virginia, our first stop was Shenandoah – I had actually never been camping before that, it was all a very new experience. We had two American kids, a Colombian kid, and a kid from South Africa… It was very liberating, and I started to see the country as it really is. At the same time, on the road, I was interviewing for jobs. I remember doing a job interview [by video phone] at a McDonalds in Idaho. I borrowed a shirt from one of my friends who dresses nicer than I do, since the interviewer could only see the top half of me… Over the course of two months, I think I applied to 200 jobs. Finally, I ended up getting a research tech job at Thomas Jefferson University in Philly.
Basking in the beauty of nature at Yellowstone
AH: What was it like adjusting to American culture?
NH: When I came to America, I had no idea what to expect, I had only heard things from my cousins who came here for college and what was on TV. One thing that I had in my mind was that I was going to try and meet as many people of different nationalities as I can. But there was a big cultural divide, how they grew up versus how I grew up. I think the road trip really helped me to understand the diversity of American people and especially during these times when people are so polarized, I reach out to that experience. We grew up seeing this version of America as the land of opportunity, the land of freedom, but America is not the government, is not their foreign policy, is not the consumerism that has taken over the world… America is more about the people that you meet here, and that’s how I see the country. America encapsulates the dichotomy of homogeneity versus heterogeneity, and I think that’s so beautiful.
The scholar/activist as a young man
AH: When did you begin to discover your interest in biology research?
NH: In Bangladesh I went to a private school that taught everything in English. The division of sciences starts in 7th grade, and biology was definitely the most interesting to me. At the same time, I was caught up in the process of deconstructing my religious identity, because I was reading biology which has hard facts about how your body works, which calls into question how life was created… I found that more fascinating than having a set answer imposed by some superior being.
Positive work environment!
AH: How did you choose your field of study for grad school, and why is it so interesting?
NH: I started reading a lot of scientific nonfiction, presenting cancer as a very complex biological phenomenon, which was fascinating to me. I also had a solid foundation in breast cancer by the time I applied for grad school and I wanted to pursue that… I had seen lots of tumors, but no mammary glands. The more I learn about the mammary gland, the more I am fascinated by it. It develops throughout life: initially it’s just a branched structure that looks like sticks; when you get pregnant, it almost flowers, with grape-like clusters that come up through alveologenesis and these alveoli then revert back to the branched structure after weaning. It’s comparable to how trees shed leaves in the Fall, except in reverse: this course of nature – the seasons that you see – the same dynamic is there in animal tissue. And all of this is happening through the lifetime, after the majority of the organs are already fully developed!
First Century – Repping Sackler at 2015 Tufts Century Ride
AH: What is one of the big challenges or controversies in your field at the moment?
NH: Traditionally, cell culture is done in two dimensions, on plates that are usually plastic – and plastic is not a natural substrate for cells to grow on, so you can’t recapitulate the same 3D environment where the cells are growing inside an organism. You can either try to mimic the natural environment as much as possible, or try to make a scaffold that is biocompatible… Cells need to be able to manipulate their environment, just as the environment should be able to provide them with physical or chemical cues to make them grow or organize in certain ways. Our lab has a very organic approach to it: we do 3D cultures in type 1 collagen, the predominant structural protein found in the mammary gland stroma. We believe that “organicism is greater than reductionism.” This is where we’re at odds with a lot of others in the cancer field, where reductionism is still the predominant philosophy. And we’re not saying it’s bad! It’s just insufficient to explain carcinogenesis.
Science is often thought of as a monolithic entity, but it is actually a complex composition of a discipline, an institution, and a community, all focused on finding truth and knowledge in data and the natural world. Science as a community consists of people of all ethnicities and from all socioeconomic classes; talent is found everywhere, and we as scientists do not and should not limit our number to those with a privileged pedigree. Science as an institution is a pillar of modern society, supporting and enabling growth and progress previously impossible to achieve. Science as a discipline is an investigative practice that demands rigor, critical analysis, and substantive evidence to support the conclusions that we draw from the data. Science as a discipline to formulate theory may be apolitical, but as an institution and a community that is an integral part of modern civic society, science cannot simply be an idle observer. Atrocities have been committed in the name of science when the idea of the pure monolith prevails and is exploited by political regimes to suppress minorities, such as the Tuskegee syphilis experiments and Nazi human trials. However, science has also been used to fight for the welfare of all people and to resist such regimes: Rachel Carson, Albert Einstein, Linus Pauling, Max von Laue all used their privilege as scientists to fight for justice and the greater good. While the scientific discipline provides a path for pure theory, we are human, each with our own biases that guide our investigation, influence our analysis, and may even blind us to the truth. Ultimately, the application of scientific theory to society bears the imprint of our ideas and our biases, and we as a community bear responsibility for the results. It is therefore imperative that we distinguish the apolitical discipline of science from the institution and community of science, which are a part of civic society and inherently political. We currently hold privileged positions in society that are at risk in the contemporary political climate. The defense of science is our moral and civic duty. Furthermore, in defending ourselves, we should also take a stand to give a voice to those who cannot do so for themselves.
This is not a temporary issue. Trump is not the only President who has or will challenge evidence-based policy and threaten the scientific community. However, it is crucial that we take action now because the dangers of climate change are imminent and we cannot afford to deny it anymore. Therefore, it is imperative that scientists come forward to educate and communicate with the public in a language and tone sufficient to start a dialogue. We start by communicating with each other, educating each other about our work. From there, we communicate and educate our family members and relatives, our friends, our communities and beyond. This has to be a grassroots movement – no top-down policy will fix the scientific literacy issue and lead American society toward a future where policies are based on hard evidence as opposed to blind faith. This is how we can give back to the public, who provide the majority of funding for our work, and ensure that science does not belong to an elite population, but in the hands and minds of the people.
This is why we are calling on you, each and every scientist, ranging from technicians to postdocs, graduate students to faculty, to action. Educate and communicate with your science. Explain why it is necessary. Even if you talk to just one person a day, that can make a difference. That is where we start. If you want to do more, organize. Rally behind policymakers who heed scientific evidence and will champion such causes. Volunteer at high schools and colleges. Take part in science festivals. Celebrate science and its achievements sans the elitism. It is not about funding, or whose research is more important. It is about making science accessible to the masses, who have tirelessly supported and benefited from our work for decades and will continue to do so. It is about rescuing science from the clutches of political partisanship. It is about freedom to communicate our science, the protection of our community, and the advancement of our society.
For too long academics have been cooped up in their self-imposed exclusive isolation from the masses. For too long we have assumed that Science exists in a vacuum. We cannot afford this axiom anymore. We have to consider the social, political, and economic forces that affect the direction of scientific research. We have a moral and civic duty to fight for what is right and to prevent the use of science to advance fascist ideology. The time to take action is now.
Here are some resources to help you take action in the short term –
Above all, talk to your family. Talk to your friends. Tell them about your work and explain why it is necessary for science to overcome partisan politics. Help educate the younger generation on the importance of scientific research. And last but not least, thank them for their support for your work.If you know of any other actions/events taking place to support Science, please let us know by leaving a comment on this post.
Stacie Clark, Molecular Microbiology, Third-Year Student: “Full of Surprises”
For this issue of Humans of Sackler, I had the chance to chat with Stacie Clark from the Microbiology program. As someone who mostly socializes within Neuroscience, it’s a real privilege for me to meet students from other programs and learn about some of the incredible, borderline-science-fiction work that’s going on right under my nose here at Sackler! Equally striking, I’ve found, is the treasure trove of unique passions and fascinating life experiences that lie just below the surface of our fellow students when we really get to talking. I’m grateful to Stacie for sharing a few of hers, and hope that you, dear reader, enjoy our conversation!
Hiking through Glacier National Park, Montana
AH: When did you realize that you wanted to pursue a career in science?
SC: My parents told me they always knew I’d end up in science. From the moment I could walk, I was outside digging for beetles and worms and building terrariums. I was in the honors science program in high school, and I did a year-long project on hand sanitizer and bacterial survival. I was working in a lab as a high school student, and realized I really liked doing that. I think I was born for science, and my parents were super-supportive. When I was growing up, we went hiking all the time, they took us to the EcoTarium in Worcester, and we were members at the Museum of Science and Aquarium. So I was always exposed to all sorts of science.
Swimming at a waterfall in El Yunque rainforest, Puerto Rico
AH: What places have you traveled to outside of Massachusetts?
SC: I studied abroad in Puerto Rico. Worcester Polytechnic Institute does this differently: they call it the IQP, Interactive Qualifying Project. The point of this project is to teach you how to work effectively in groups and communicate with people outside the university. I worked in the rainforest in Puerto Rico, and we did a project evaluating stream crossings. We wanted to look at how their bridges were affecting stream flow and water quality, so we got to hike all through the [El Yunque] rainforest and evaluate all these different stream crossings. We got to see parts of the rainforest that no one gets to see!
With Pablo the capuchin monkey in Costa Rica
AH: What did you do between graduating from WPI and starting your Ph.D. at Sackler?
SC: Before I started grad school, I had always wanted to work with exotic animals. So I literally just Googled ‘volunteer experience in Costa Rica’ and this small remote place in Costa Rica popped up. I booked a two-week trip, went by myself back-packing in Costa Rica, and volunteered at an animal rehabilitation center. It was quite an adjustment: I was on a mountainside in southern Costa Rica, and it got pitch-black at 6 o’clock at night. I would go into the rehabilitation center, clean the cages, prep all the food, and then feed and play with the animals. The monkeys were my favorite, and there was also an anteater. His name was Gomer; if you went into his cage and just yelled out ‘Hey Gomer!’ he’d come crawling out, and he loved being held. We’d do enrichment activities for some of them too – so with the anteater, I would walk with him out in the jungle and let him go searching for termites and ants on his own, and then I’d go bring him back to his cage. I think everyone should go on at least one trip by themselves, because you learn a lot about yourself and it’s just a good experience!
At the beach with Kid Rock
AH: What do you like to do when you’re not working in the lab?
SC: I volunteer at the animal shelter in Quincy; I’ve been doing that every Monday for four years. I take the dogs out for walks, play with them, cuddle with them if they want to… They only get to go outside twice a day, that’s the only time they get to really play with people. I understand that work-life balance is really important to your mental health, so volunteering on Mondays is the one thing that I won’t let grad school take away from me. It’s something that I do for me that I enjoy – and I’m also a big dog person.
Group photo with the Leong Lab (middle row, second from right)
AH: There are so many disciplines within biology – what got you interested in studying bacteria specifically?
SC: I’ve always been fascinated that an organism so small can have such a large impact on humans – that still blows my mind! They’re incredible organisms that can mimic the proteins we have, which I find pretty amazing. We’re full of bacteria, they do a lot for us – and the microbiota is a huge field now. Everyone is fascinated in studying microbiota and the impact they have on our health in general.
Out on the town with friends
AH: What particular species of bacteria do you study, and what makes it so interesting?
SC: Yersinia pseudotuberculosis is a model pathogen that we use to study community behavior of bacteria within its host. Yersinia can establish a distinct niche within the spleen of a mouse, and once it forms a microcolony, it can replicate to high numbers despite the presence of the immune system. You get a recruitment of innate immune cells to the site of infection, triggering a response in the bacteria to create specialized populations within that distinct cluster; I always thought that was cool, the response between the bacteria and the host cells.
Here at Maine Medical Center Research Institute, we are very happy to be supporting Tufts trainees and working with many Tufts investigators here and in Boston to provide core facility services such as transgenic mouse generation.
Did you know that many of our core facilities were established at Maine Medical Center through a special NIH program, the Institutional Development Award (IDeA) Program? The IDeA program was established by Congressional mandate in 1993 to help develop research infrastructure to support biomedical research in 23 states that historically have had a low level of NIH funding. Maine is one of those states. In fact, there was a time when 50% of NIH funding went to researchers in 5 states (Massachusetts being one of those heavily funded states!), while the 23 IDeA eligible states together only received about 5% of all NIH funds. Over the last 23 years, NIH investment in biomedical research in Maine has contributed to a burgeoning biotech scene (http://www.mainebioscience.org/access_resources/bioscience-map-of-maine/) and a highly collaborative network of research institutes.
One of the components of the IDeA program is the Centers of Biomedical Research Excellence (COBRE). Maine Medical Center has been fortunate to have received two COBRE awards since 2000, one with the theme of Vascular Biology, and one in Stem and Progenitor Cell Biology. These awards have supported the recruitment of new junior investigators to Maine Medical Center (with appointments at Tufts University School of Medicine), and also the establishment and expansion of our core facilities. Please visit our website at mmcri.org, and find “Core Facilities” under “Research Services & Resources” to see if we provide services that could be useful to your research!
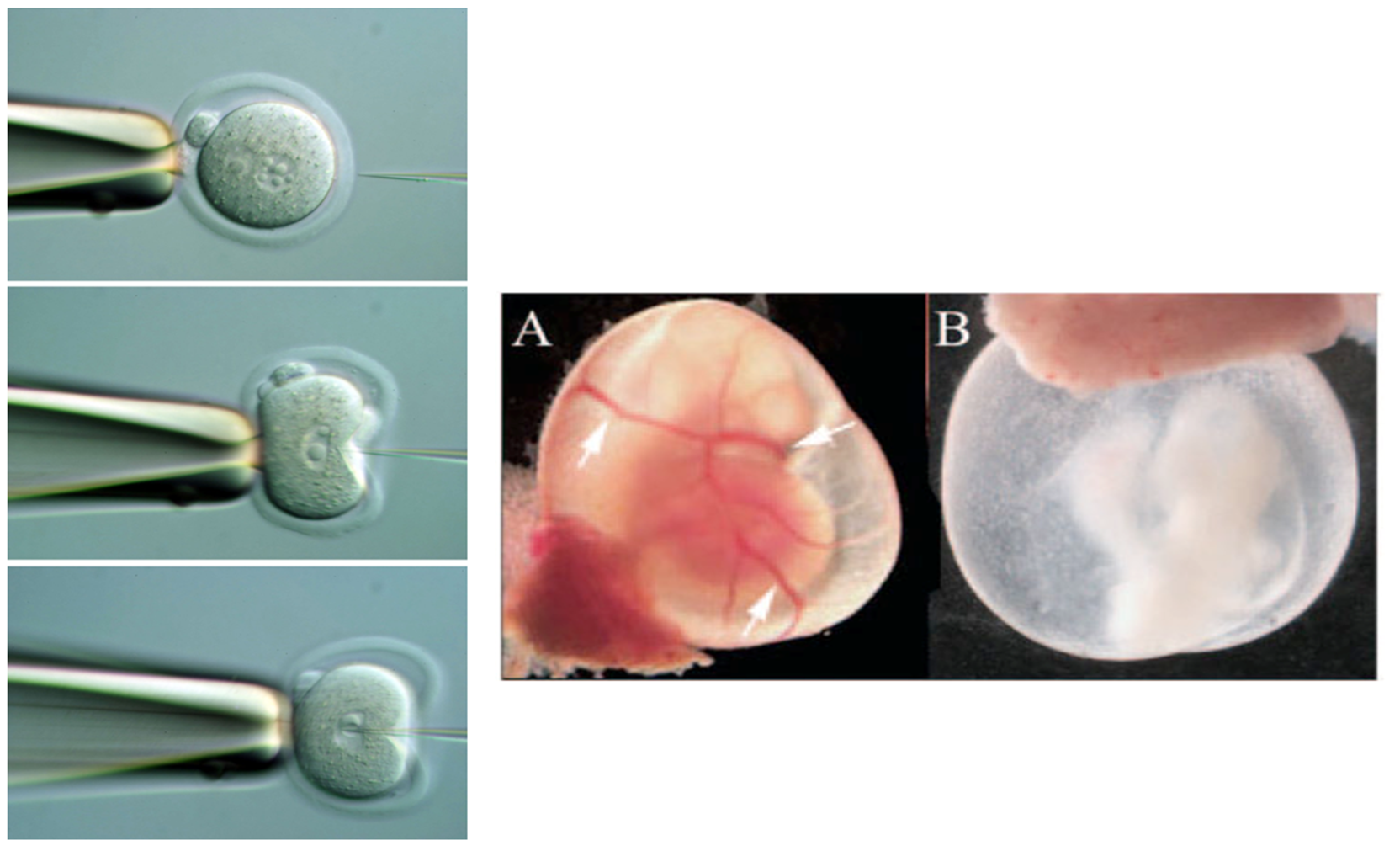
Microinjection of mouse fertilized oocyte. Our Mouse Transgenic Facility performs genome modification using standard transgenesis, gene targeting in ES cells, or CRISPR/Cas. In 2017, we will start to offer services for CRISPR/Cas project design and sgRNA synthesis.
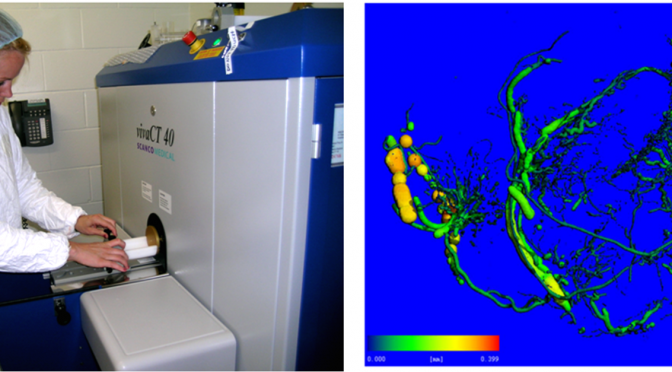
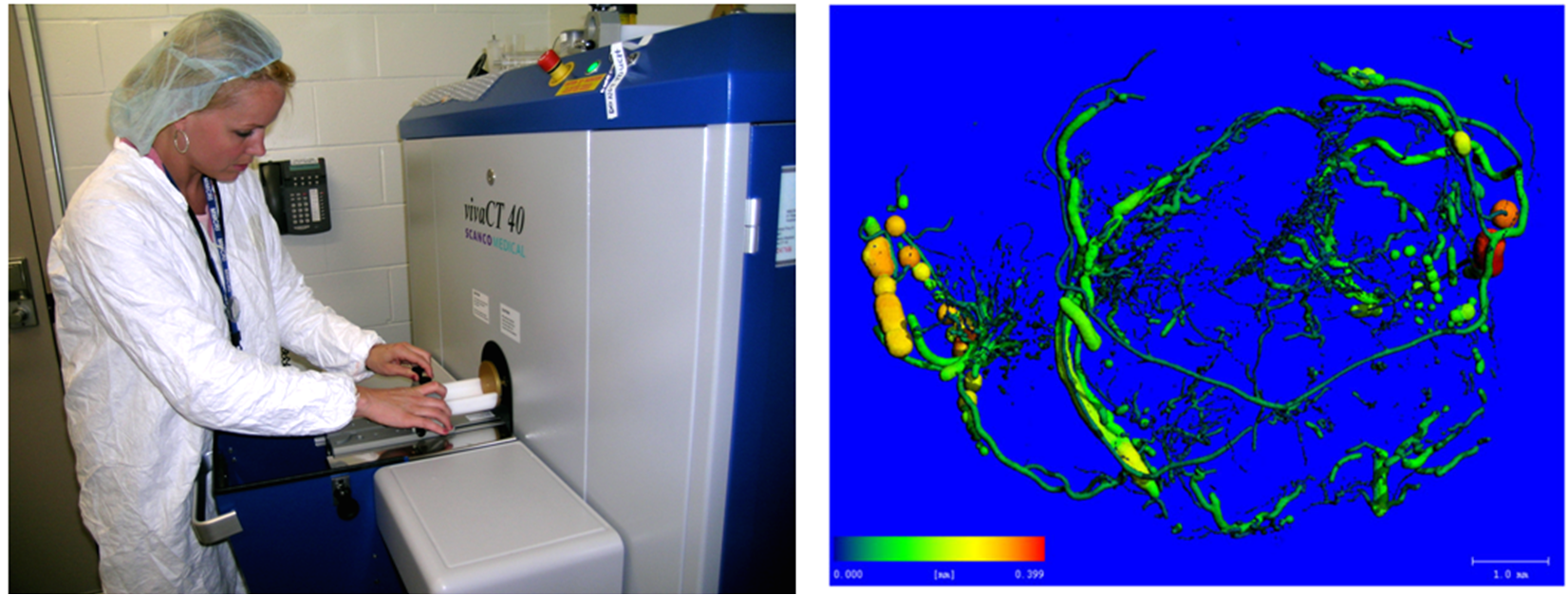
Imaging by microCT. We run a Scanco vivaCT40 for microCT imaging of bone, teeth, fat, and the vasculature. Image, above right, shows microfil perfusion of the vasculature of a tumor xenograft, used to quantify and measure tumor angiogenesis.
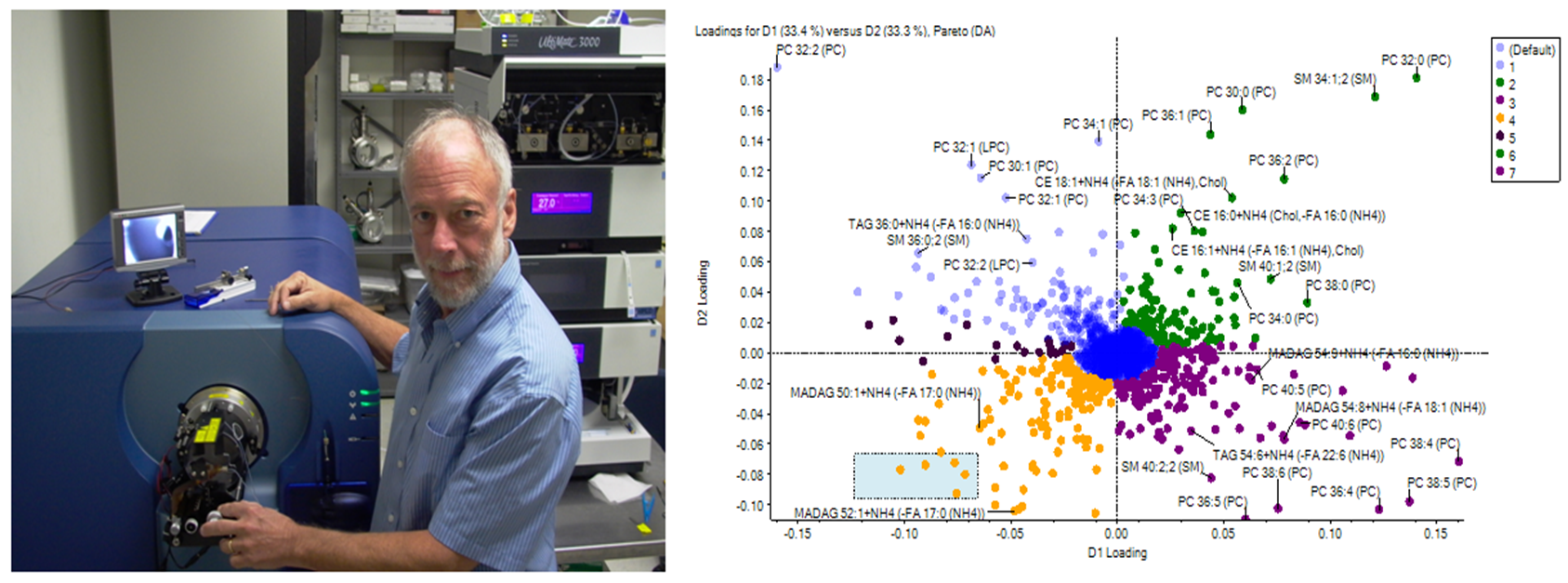
Proteomics and Lipidomics Core Facility. We run a mass spectrometry resource with state-of-the-art protein and lipid profiling capacity. Recent studies include experiments to study tissues including adipose tissues and the skeleton, and how their protein and lipid content changes during metabolic disease.
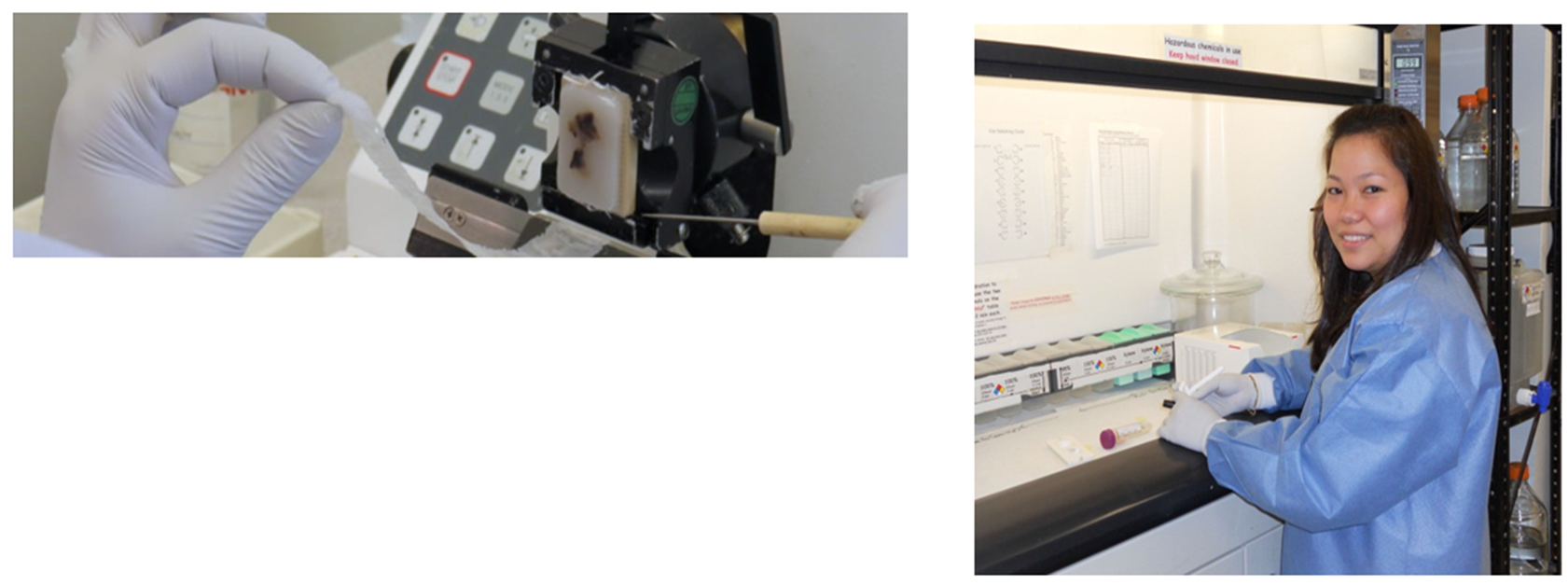
Histopathology Core Facility. We provide full services for tissue processing, embedding, sectioning, routine histology, and immunostaining. We work closely with our Maine Medical Center Biobank to generate tissue arrays for screening of human disease specimens from patients.
In January 2015, President Obama announced the launch of the “Precision Medicine Initiative”, proclaiming it to usher in “a new era of medicine that makes sure new jobs and new industries and new lifesaving treatments for diseases are created right here in the United States.” In addition, he remarked that the promise of this initiative laid in “delivering the right treatments, at the right time, every time to the right person”. This initiative, with bipartisan support in the Congress, provided a total of $215 million investment in 2016 for the NIH, along with the FDA and the Office of the National Coordinator for Health Information Technology (ONC), with a large portion of the money ($70 million) awarded to NCI to “scale up efforts to identify genomic drivers in cancer and apply that knowledge in the development of more effective approaches to cancer treatment”. The initiative doesn’t stop at the genome level, as Dr. Francis Collins, Director of the NIH, pointed out in an interview with PBS News Hour, and is meant to provide information about environmental exposures, lifestyle choices and habits and pretty much everything that can affect one’s health. Given the mass of information that will be generated (the initiative aims to enlist 1 million volunteers for its cohort), it is no surprise that patient privacy issues, as well as database infrastructure, are major concerns in this mammoth undertaking.
In addition to this initiative, the US government also launched its “Cancer Moonshot Program” a year later in January 2016. This program, under the leadership of Vice President Joe Biden, and with the help of an expert panel, the “Cancer Moonshot Task Force”, aims to “make more therapies available to more patients, while also improving our ability to prevent cancer and detect it at an early stage.” Since cancer is widely accepted to be a genetic disease, it seems fitting to serve as the poster child for an initiative that aims to cure and prevent diseases based on tailoring therapy for an individual using personal genetic information.
Tied to these two initiatives is also the latest approach to clinical trials at the NCI, commonly termed as “basket trials”. Based on findings from exceptional case reports where patients treated with drugs not commonly used for that type of cancer, the NCI was encouraged to try out drugs traditionally reserved for particular types of cancer for the ones that they weren’t developed for; thus, the Molecular Analysis for Therapy Choice (MATCH) and the Molecular Profiling-Based Assignment of Cancer Therapy (MPACT) trials were incorporated into the Precision Medicine initiative. The NCI-MATCH trial aims to sequence tumor biopsy specimens from ~6,000 patients to identify mutations that will respond to targeted drugs selected for the trial; these drugs are already approved by the FDA for certain cancer types or are being tested in other clinical trials. On the other hand, the MPACT trial will compare whether patients with solid tumors fare better with targeted therapy vs non-targeted therapy.
The NCI-MATCH trial explained. Source: National Cancer Institute website.
Despite the initial fanfare, the recently released NCI-MATCH major interim analysis report does not paint a pretty picture for the trial’s outcome. While the enrollment was higher than expected (795 people registered in first 3 months compared to the projected 50 patients/month) and the labs were able to sequence most of the tumors (87%), it was also found that “most of the actual mutation prevalence rates were much lower than expected based on estimates from The Cancer Genome Atlas and other sources”. In fact, the overall expected mutation match rate was adjusted to 23% for the 24 treatment arms in the study as it continues.
While no endpoint has yet been reached to draw conclusive remarks about this trial, data available from other clinical trials that have taken a similar approach do not seem favorable. In the SHIVA trial, a randomized phase II trial carried out in France where 99 patients were treated based on identified mutation(s) compared to 96 patients treated with drugs of their physicians’ choice, median progression-free survival was 2.3 and 2 months, respectively. Current clinical data on patients with relapsed cancers, a major focus of the MATCH trial, do not seem favorable either. As Dr. Vinay Prasad, a haematologist-oncologist at Knight Cancer Institute, points out, only 30% of such patients respond to drugs based on biological markers and the median progression-free survival is 5.7 months. Based on this response rate, he estimated only 1.5% of patients with relapsed and refractory solid tumors to benefit from the precision medicine approach.
In a review of current clinical trials and past trials that have used the targeted therapy approach, Tannock & Hickman (NEJM, 2016) warn about the limitations of such an approach – heterogeneity and clonal evolution of cancer cells when challenged with targeted therapy, the inconsistency between expected and clinically achievable levels of inhibition of candidate molecules and of course, the efficacy of such therapies compared to currently available, standard but effective therapies such as aromatase inhibitors for breast cancer. While one can argue that heterogeneity in tumors can be countered with combination targeted therapy, the authors point out that “combinations of molecular targeted agents that target different pathways have often resulted in dose reduction because of toxic effects… in a review of 95 doublet combinations in 144 trials, approximately 50% of the combinations could use the full doses that were recommended for use as single agents, whereas other doublets required substantial dose reductions.” Even if it is possible that intratumoral heterogeneity can be countered with combination targeted therapy, a much-overlooked point in this initiative is the cost of such treatment strategy, considering the exorbitant costs of targeted cancer therapy. There already exists a disparity among cancer patients from a socio-economic standpoint and this initiative does little to address how to bridge such a gap. Questions such as how many drugs will a patient have to take, especially in cases of tumors that are highly heterogeneous, such as glioblastoma multiforme and how that would affect the living standard of a patient need to be considered before heralding a victory for the precision oncology approach even if the MATCH trial outcomes are favorable.
In another recent study, Dr. Victor Velculescu and his team from Johns Hopkins showed that sequencing only tumor genetic data can lead to false positives. After analyzing 815 cancer patients’ tumor sequencing data and comparing that data to the one from the patients’ healthy tissue, they found that 65% of genetic changes identified with tumor-only sequencing data were unrelated to the cancer and therefore, “false positives”. The team also found that 33% of mutations, which are targets of currently available drugs, were also false positives when the patient’s germline genome was compared to the tumor genome; this affected 48% of the patients in their cohort.
The paradigm behind the MATCH trial, and in general the Precision Medicine initiative, seems to be blind to an obvious aspect of biology – context matters, and more so, in case of mutations that are deemed to be “carcinogenic”. As outlined in a recent paper by Zhu et al (Cell, 2016) and the famous “bad luck” paper by Tomasetti and Vogelstein, it appears that the stem cells and their differential regenerative properties in different tissue types are responsible for the differential rates of carcinogenesis in various tissue types, a finding that again, buttresses the idea that tissue specificity matters. In fact, Iorio et al (Cell, 2016) was able to show just that in the context of pharmacogenomic interactions of currently available cancer drugs with data available from patient samples in the TCGA and other databases. Using a big data and machine learning approach, the authors developed a logic-based model that would predict the efficacy of any drug that is either approved or undergoing clinical trials against the mutation it is intended for in different cancer types ,which is essentially the basis of the MATCH trial. Surprisingly, it appeared that tissue specificity determined the pharmacological agents’ effects on the intended molecular targets; more specifically, only one drug interaction (out of 265 drugs tested) was found to be significant in multiple cancer types, which may sober up the expectations from the MATCH trial outcome. Therefore, using a blanket approach to target mutations in various tissue types without consideration to their environments can seem futile in the light of such findings.
The evidence from all these basic science and clinical studies raise the question of whether precision medicine is doomed to fail. While the gene-centric view of disease etiology have deepened over the years since the completion of the Human Genome Project, does this evidence point to the necessity of another paradigm in our understanding of cancer and other complex diseases, whose cures have been presumed to lie in genetic aberrations and molecular targets? An even more concerning question, relevant in this era of big data, is whether we actually understand what the data is telling us, as the prominent cancer researcher, Dr. Robert Weinberg, admits that “while data mining, as it’s now called, occassionally flags one or another highly interesting gene or protein, the use of entire data sets to rationalize how and why a cancer cell behaves as it does is still far beyond our reach”. A strong critic of the initiative, Dr. Michael Joyner from Mayo Clinic, opines that while “hundreds of genetic risk variants with small effects have been identified…But for widespread diseases like diabetes, heart disease and most cancers, no clear genetic story has emerged for a vast majority of cases” and that “when higher-risk genetic variants are found, their predictive power is frequently dependent on environment, culture and behavior”.
The success of Precision Medicine Initiative, and in particular, the precision oncology approach, ultimately rests on whether it can stem and curb deaths resulting from cancer and other complex diseases, based on molecular targeted therapy. Unfortunately, it appears that large scale public health initiatives have done more to that end (e.g. – tobacco control has largely cut down rates of lung cancer incidence, diet and exercise can cut down the risk of converting pre-diabetes to diabetes by nearly two-thirds), compared to what targeted therapy have achieved. However, it seems that such public health success was overlooked by the Cancer Moonshot panel as in February 2016, right after the program was announced, public health researchers across the country had to urge the Vice President to make prevention a bigger focus in controlling cancer incidence in the population, rather than just trying to find a cure. This approach should have been incorporated into a billion-dollar initiative by default, one would think, but this didn’t seem to be the case and one must wonder why.
In order for this huge, publicly-funded initiative to achieve more than just lukewarm outcomes and to actually become a breakthrough it is promised to be, the Precision Medicine initiative needs to break free of the gene-centered tunnel vision and incorporate all factors that affect an individual’s health, such as lifestyle choices and environmental exposures, as Dr. Collins boasted it to be. While this initiative is only at its infantile stage, changes based on clinical trial and basic science evidence should be made early enough so that favorable outcomes can be achieved and does not require the government to stage another public bailout as it did for the failing banks and wall street corporations back in 2008 when they were deemed to be “too big to fail”.
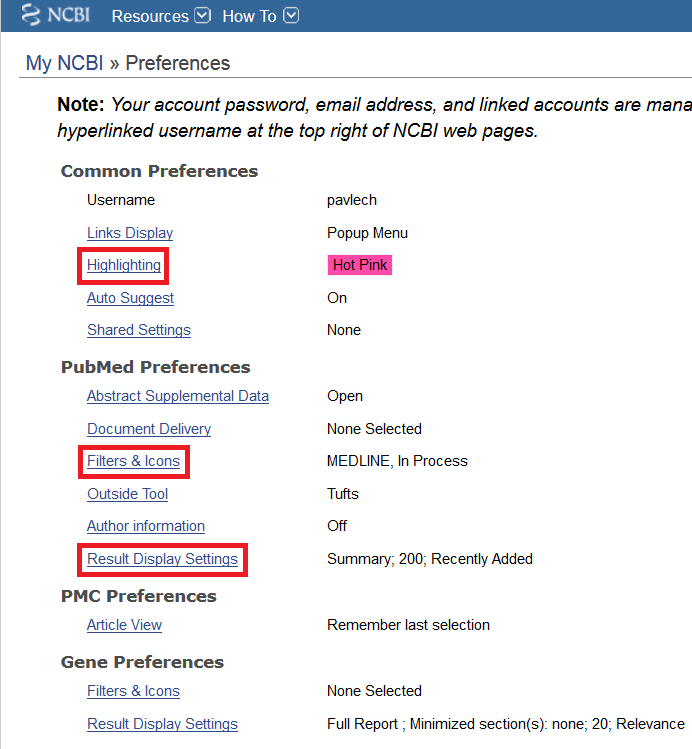
You can customize your preferences to make searching PubMed and other NCBI databases easier. Log in to your My NCBI account (see Insight March 2016 for details on creating a My NCBI account) and click the ‘NCBI Site Preferences’ link in the top right corner of the homepage.
Here are a few preferences that you may want to adjust:
Highlighting: Highlights your search terms in a set of results, making scanning for relevant articles more efficient.
Filters & Icons: Personalized filters displayed in the right-hand column on results page. I recommend adding the MEDLINE filter, which limits results to articles that have had MeSH terms applied to them. To do so, click on the ‘Filters & Icons’ link on the Preferences page, and on the page that opens, select the ‘Properties’ radio button. Enter ‘MEDLINE’ in the search with terms box, then check the box next to MEDLINE. You can also add the ‘Find it @Tufts’ button, which enables you to access the full text of an article through Tufts Libraries. Adding this button to your NCBI account would obviate the need to access PubMed through the Hirsh Health Sciences Library website. To add the ‘Find it @Tufts’ button, select the ‘LinkOut’ radio button on the Filters & Icons page. Then, enter ‘Tufts University’ in the search box and check the link icon box next to Tufts University Hirsh Health Sciences and Veterinary Libraries.
Outside Tool: A simpler method of adding the ‘Find it @Tufts’ button to your account preferences. Click the ‘Outside Tool’ link on the Preferences page. On the page that opens, select the radio button next to ‘Tufts’.
Result Display Settings: You can choose the format (summary or abstract) in which results are displayed, how results are sorted (I do not recommend changing this from the default, recently added), and the number of items per page (I prefer 200, so I don’t have to click through multiple pages).
These are just a few of the preferences that you can adjust in your My NCBI account. You can also explore customized settings for other NCBI databases, such as Gene.